
Low-dose atropine has become one of the most discussed pharmacological treatments in childhood myopia management. It is familiar to ophthalmologists, relatively simple to prescribe, and supported by a growing body of randomized clinical trials. With the European approval of Ryjunea®, low-dose atropine has also entered a new regulatory phase (1, 2).
The central question is no longer simply whether low-dose atropine can reduce myopia progression. It can reduce progression in many trial settings, although the magnitude of benefit varies. The more relevant question is whether the chosen dose sufficiently modifies the axial growth trajectory of the child in front of us.
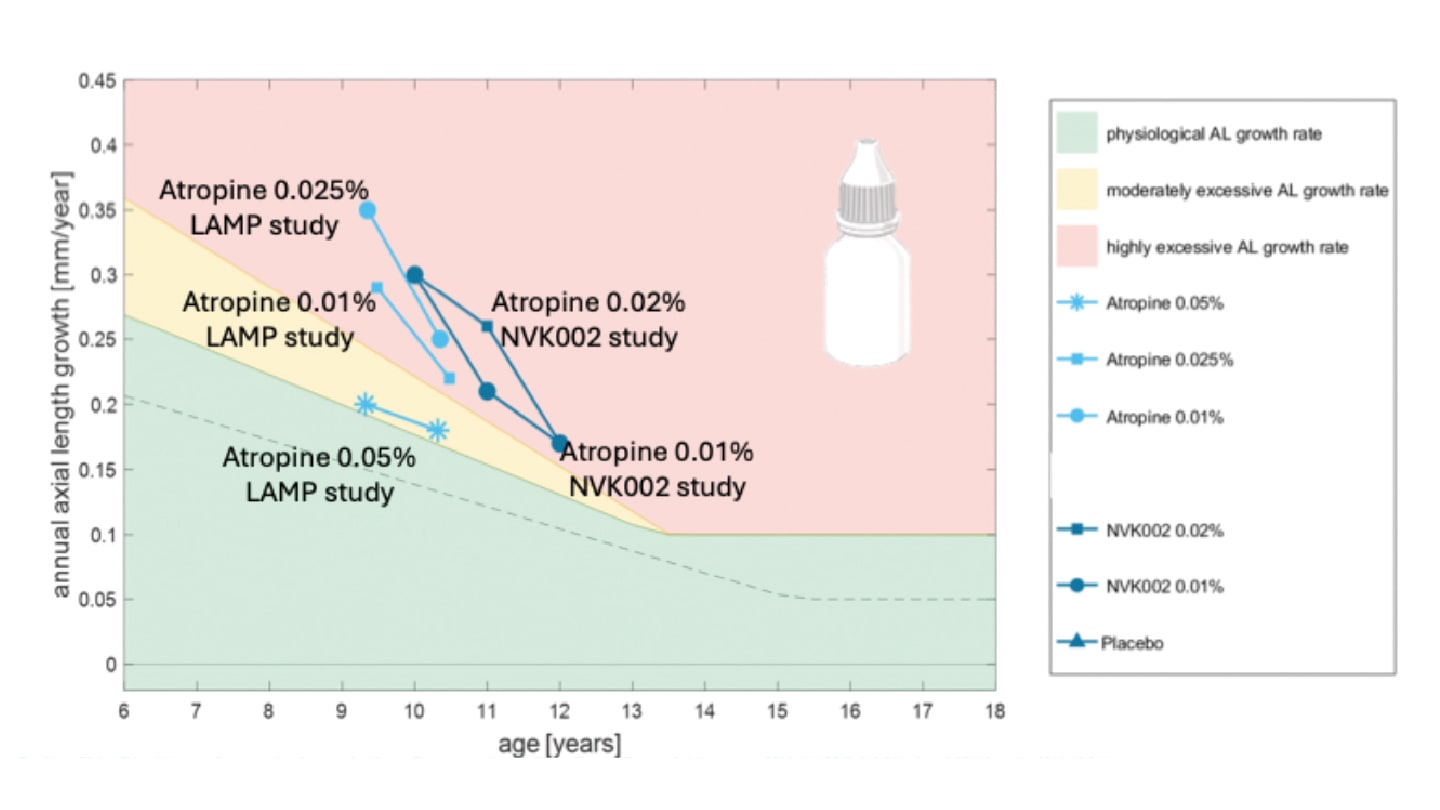
A treatment effect may not be equivalent to treatment success. A clinically meaningful question is whether low-dose atropine moves excessive axial elongation closer to age-appropriate physiological growth. At present, however, this should be understood as an emerging interpretive framework rather than a fully validated regulatory endpoint for atropine trials. Most existing atropine studies were not prospectively designed to test treatment success against age-matched physiological growth targets (3, 4, 5).
Low dose is not one dose
The term “low-dose atropine” is convenient, but imprecise. A 0.01% formulation is not biologically equivalent to 0.025%, 0.03% or 0.05%. Grouping these concentrations under one label risks hiding clinically relevant differences.
The LAMP study provided the clearest dose-response signal among low atropine concentrations. Atropine 0.05%, 0.025% and 0.01% all reduced myopia progression, but the effect was concentration dependent, with 0.05% generally showing the strongest efficacy over one and two years (6, 7). The 2025 International Myopia Institute intervention report similarly concluded that 0.05% was the most effective among the lower-dose concentrations (4).
Intermediate concentrations also deserve attention. A one-year prospective, non-randomized clinical study of 0.03% atropine reported lower axial elongation than in the control group, with mean axial length change of 0.19 mm versus 0.31 mm and refractive progression of −0.34 D versus −0.60 D. However, adverse events were reported in 35% of treated children and 16% discontinued treatment because of these adverse events, although none were severe (8).
This supports the idea that low-dose atropine should be understood as a dose range, not as a single treatment category. The practical consequence is that dosing strategy deserves as much scrutiny as trial efficacy.
Why the evidence resists a simple recommendation
Review tables of atropine trials often summarize absolute effects, percentage effects, and statistical significance, as illustrated by Farassat’s overview of topical atropine trials since ATOM (9). These data are useful, but they are not enough.
A p value tells us whether a difference within one study is unlikely to be due to chance. It does not tell us whether one trial can be directly compared with another, nor whether the treated eye has reached a clinically desirable growth trajectory. Different studies start from different baseline ages, baseline progression rates, inclusion criteria, formulations, follow-up periods, measurement protocols, and adherence patterns. Even absolute treatment effects can be misleading if they are detached from the child’s starting point (3).
This is why the current evidence does not support a simple universal recommendation such as “use 0.01% atropine for all children” or “start every progressing child at 0.05%.” The trial results are too heterogeneous for that. Some studies show meaningful refractive effects but weaker axial signals; others show modest axial benefit without a consistent refractive effect; and some show little or no advantage over placebo. These differences are not just statistical noise; they reflect variation in baseline progression, formulation, endpoint hierarchy, adherence, and follow-up.
Current trial endpoints (refractive progression, axial elongation, responder proportions and percentage efficacy) remain important and should not be discarded. But they may need to be supplemented by trajectory-based endpoints that are clinically interpretable for individual children. Examples include annualized axial growth relative to age, time within a predefined physiological growth corridor, time to treatment failure, or an Emmetropic Progression Ratio, as discussed in the IMI 2025 report (4).
Such endpoints require prospective validation before being treated as measures of treatment success. The available evidence suggests that low-dose atropine can reduce axial growth, but most trials were not designed to test prospectively defined growth targets. That remains a key question for future research.
The 0.01% problem
The evidence base for 0.01% atropine is now substantial, but it should be read carefully. The IMI 2025 report identified 21 randomized clinical trials of 0.01% atropine. The median axial-length efficacy was approximately 0.08 mm after one year and 0.12 mm after two years (4). That is a real but modest effect, and its adequacy depends on baseline risk and treatment target.
This distinction matters because 0.01% atropine has often been treated as the “safe default.” While safety and tolerability are important, a well-tolerated treatment that does not sufficiently slow axial elongation may reassure the clinician more than it benefits the patient.
Recent trials show why oversimplification is risky. CHAMP/NVK002 supported a treatment effect for 0.01% atropine over three years, while 0.02% did not meet the prespecified primary responder endpoint, although it reduced axial elongation (10). PEDIG, by contrast, found no meaningful benefit of 0.01% atropine over placebo for myopia progression or axial elongation over two years (11). MOSAIC showed that 0.01% atropine was safe and well tolerated and reduced axial elongation over two years, although treatment effects were not uniform across outcomes (12).
This interpretation is consistent with recent narrative syntheses (13). For clinical practice, 0.01% atropine is best understood as a modest option whose adequacy depends on baseline risk, endpoint and treatment target.
Ryjunea® and the axial-length question
Ryjunea® is an authorized atropine sulfate 0.1 mg/ml formulation, equivalent to 0.01%, for slowing myopia progression in pediatric patients. According to the European Medicines Agency, treatment may be initiated in children aged 3–14 years with documented progression of at least 0.5 D per year and myopia between −0.5 D and −6.0 D (1, 2).
A regulated formulation represents a clear advance over variable compounded preparations by improving standardization, quality control and pharmacovigilance. However, this addresses uncertainty about the formulation, not uncertainty about whether 0.01% provides sufficient efficacy to alter the child’s axial growth trajectory (1, 2, 14).
The pivotal STAR study tested atropine sulfate 0.01% and 0.03% against vehicle in children aged 3–14 years. At 24 months, both concentrations significantly reduced refractive progression compared with vehicle. However, the available axial-length analyses showed numerical but non-significant effects for 0.01%, making the axial signal less persuasive than the refractive signal (15).
The EMA public assessment report identifies ongoing uncertainties regarding long-term clinical effects, tapering and rebound, with further 48-month results requested as a post-authorization efficacy study (14). This does not invalidate the approval. But it matters for clinical interpretation. If our treatment target is the growing eye, then axial length must remain central.
Start with efficacy, then adjust for tolerability
In children for whom pharmacological treatment is indicated and meaningful axial control is the clinical aim, a purely stepwise approach, starting at 0.01% and escalating only after insufficient control, may be too conservative. Where local regulation and availability allow, a pragmatic alternative is to start with 0.05% atropine, the low-dose concentration with the strongest efficacy signal in LAMP, and then adjust according to tolerability (6, 7, 4).
This is not a rigid concentration-based algorithm. It is a tolerability-guided de-escalation strategy: begin with a biologically more persuasive pharmacological signal, assess tolerability after approximately two weeks, and reduce the dose if symptoms such as photophobia, near blur, reading difficulty, headache, or ocular-surface discomfort interfere with school, reading, or adherence.
The aim is not to force every child to remain on 0.05%, but to identify the strongest tolerated concentration early. Axial efficacy cannot be judged after two weeks; it requires structured follow-up, ideally with the same biometer and annualized axial-length assessment. This strategy is clinically plausible but still requires prospective testing.
What evidence do we need next?
Future trials should prospectively define what constitutes clinically adequate axial control. This may include age-adjusted axial growth targets, predefined physiological growth corridors, time-to-treatment-failure designs, or responder definitions based on axial growth rather than refraction alone.
Such studies should include standardized axial-length protocols, sufficient follow-up beyond two years, treatment cessation phases, adherence assessment, and stratification by baseline risk. They should also compare dosing strategies, including lower-dose initiation with escalation versus 0.05% initiation with tolerability-guided de-escalation.
This would not replace conventional endpoints. It would make them more clinically interpretable. The aim is to understand not only whether atropine changes the average trial result, but whether it changes the developmental trajectory of the individual child.
Conclusion
Low-dose atropine has earned its place in myopia management, but it should not become a substitute for biological judgement. Ryjunea® provides an authorized 0.01% atropine option for defined pediatric patients with progressive myopia, and that is a real regulatory advance.
The available studies point in different directions: effects are real in some settings, modest or inconsistent in others, and not always equally persuasive for refraction and axial length. In children for whom pharmacological treatment is indicated, a pragmatic strategy is to start with a biologically effective concentration such as 0.05%, assess tolerability early, and reduce the dose if necessary. Future studies should test whether such a tolerability-guided de-escalation strategy achieves better axial-growth control than starting low and escalating late.
References
- European Medicines Agency, “Ryjunea: EPAR – Medicine overview,” EMA/119451/2025 (2025).
- European Medicines Agency, “Ryjunea 0.1 mg/ml eye drops, solution: Summary of product characteristics” (2025).
- NA Brennan et al., “Efficacy in myopia control,” Prog Retin Eye Res, 83, 100923 (2021). PMID: 32979579.
- MA Bullimore et al., “IMI – Interventions for controlling myopia onset and progression 2025,” Invest Ophthalmol Vis Sci, 66, 39 (2025).
- H Kaymak et al., “Emmetropic eye growth as treatment goal for myopia management,” Ophthalmologe, 119, 528 (2022). PMID: 35067663.
- JC Yam et al., “Low-Concentration Atropine for Myopia Progression study: A randomized, double-masked, placebo-controlled trial of 0.05%, 0.025%, and 0.01% atropine eye drops,” Ophthalmology, 126, 113 (2019). PMID: 30514630.
- JC Yam et al., “Two-year clinical trial of the Low-Concentration Atropine for Myopia Progression study: Phase 2 report,” Ophthalmology, 127, 910 (2020). PMID: 32019700.
- D Simonaviciute et al., “Efficacy and safety of 0.03% atropine eye drops in controlling myopia progression: A one-year prospective clinical study,” J Clin Med, 13, 3218 (2024). PMID: 38892695.
- N Farassat, “Topical atropine for myopia control: A review,” Klin Monbl Augenheilkd, 241, 1134 (2024). PMID: 39125101.
- K Zadnik et al., “Efficacy and safety of 0.01% and 0.02% atropine for the treatment of pediatric myopia progression over 3 years: A randomized clinical trial,” JAMA Ophthalmol, 141, 990 (2023). PMID: 37603754.
- MX Repka et al., “Low-dose 0.01% atropine eye drops vs placebo for myopia control: A randomized clinical trial,” JAMA Ophthalmol, 141, 756 (2023). PMID: 37440213.
- J Loughman et al., “Myopia outcome study of atropine in children: Two-year result of daily 0.01% atropine in a European population,” Acta Ophthalmol, 102, e245 (2024). PMID: 37672874.
- A Grzybowski, C Lanca, “Management of myopia: A mini-review,” Med Hypothesis Discov Innov Ophthalmol, 15, 19 (2026).
- European Medicines Agency, “Ryjunea: EPAR – Public assessment report,” EMA/134905/2025 (2025).
- M Korenfeld et al., “Study of Atropine to Reduce (STAR) myopia progression in children: 24-month results of a randomized, double-masked, vehicle-controlled trial of atropine sulfate 0.01% and 0.03%,” Ophthalmol Ther (2026). DOI: 10.1007/s40123-026-01341-0.
