I have stopped implanting traditional monofocal IOLs in my practice. All cataract patients receive at least an enhanced monofocal IOL, and if their expected residual astigmatism exceeds 0.5 D, they also receive a toric lens. About 85% of our patients also choose to correct presbyopia, and these patients end up being about equally split between increased range of focus (IRoF) and full range of focus (FRoF) IOLs. There are only two price points for cataract surgery – with or without presbyopia correction – at our clinic. This model is somewhat unusual, given that we are a private clinic and patients are paying out of pocket or with insurance, rather than relying on the national health care system.
In choosing between the “increased” or “full” range of focus, safety is the first criterion. In patients with mild pathology, such as early glaucoma, very early epiretinal membrane development, or retinal pigment epithelial changes, we might expect some loss of contrast sensitivity in the future, so I believe an IRoF lens is a safer choice for those patients. For patients who are otherwise good candidates for any presbyopia-correcting IOL, my decision trigger is their response to the question, “How much would you be bothered if you experienced night vision problems or halos when driving?” If the patient is no longer driving or not particularly concerned about night vision symptoms, I would implant a FRoF lens. If they are hesitant about the potential for night vision problems, I opt for an IRoF lens.
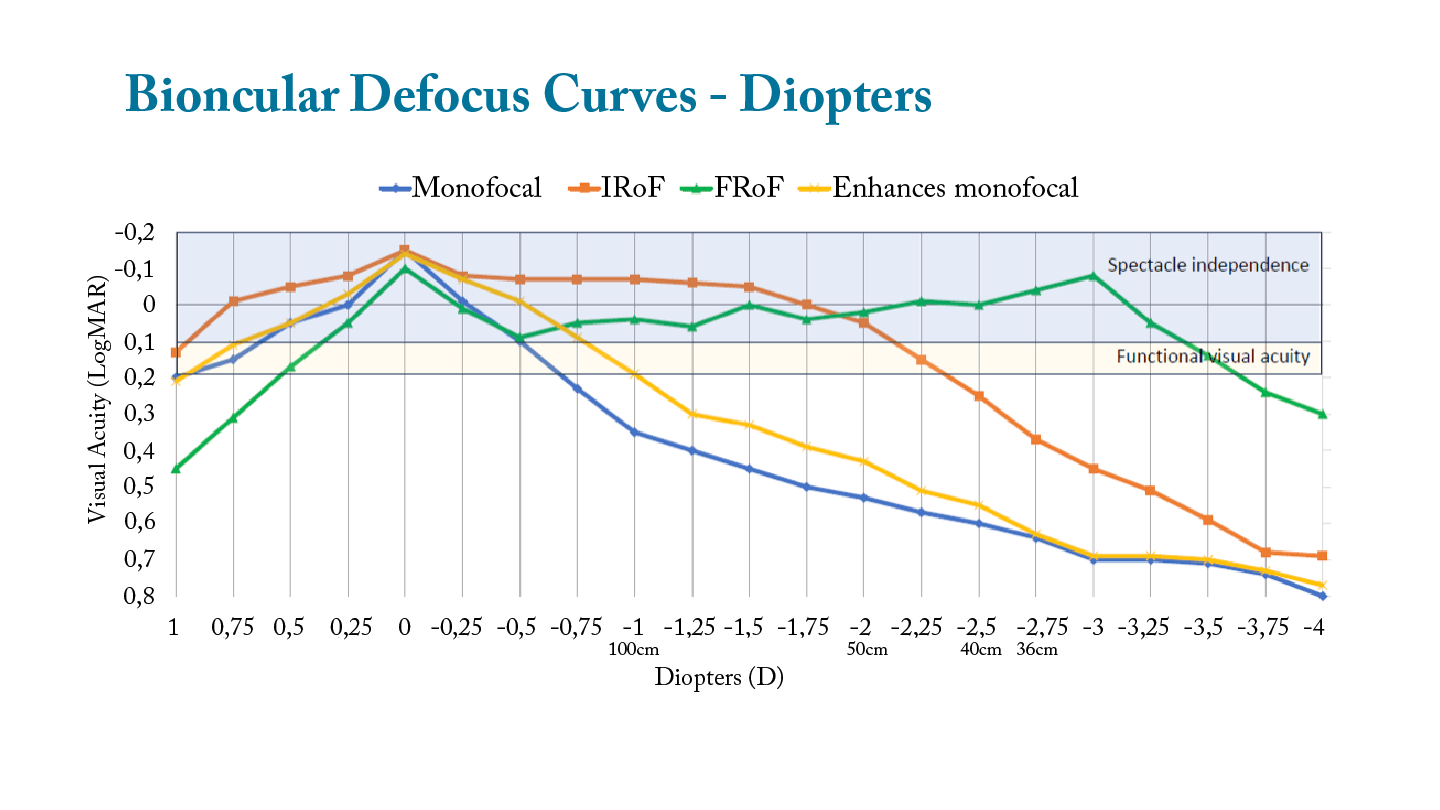
I show patients a comparison of the binocular defocus curves achieved in our clinic for all four types of lenses (Figure 1). While monocular defocus curves are used in scientific studies to illustrate the performance of an IOL, patients’ real-world experience is a binocular one, so that’s what I discuss. Distance is more relatable to patients than diopters, so I include the distance that corresponds to each level of defocus on the graph. I tell them that the portion of the graphed line they see in the blue zone at the top represents the distances at which they can expect to be spectacle independent, and the yellow zone represents the distances where they may need readers for some tasks but can still be pretty functional. Having this discussion preoperatively helps set clear expectations for the visual performance that patients can expect postoperatively.
There are important differences within each of these IOL categories. Recently, I conducted a comparative evaluation of all four of the IRoF IOLs that I was using at the time: TECNIS Symfony (Johnson & Johnson), AT Lara (Zeiss), Acrysof Vivity (Alcon), and TECNIS PureSee (Johnson & Johnson). While these lenses share commonalities in the degree of spectacle independence they provide, they take a variety of approaches to extending the range of focus, as can be seen in aberrometry maps (Figure 2) generated by the Osiris aberrometer (CSO Italia). The TECNIS Symfony and AT-Lisa IOLs have diffractive optics, with continuous dioptric power changes across the full optic to extend the range. The Vivity and TECNIS PureSee lenses utilize refractive optics, extending the range through zonal optics.

For this study, I evaluated 50 eyes of 25 patients in each IOL group. All patients were plano or nearly so (sphere ±0.25 and very low cylinder). Essentially, we selected patients who would be expected to have optimal performance and whose near vision would not be helped or hindered by any residual sphere.
Three months after surgery, we assessed visual acuity without spectacles at three different distances (400 cm, 60 cm, and 45 cm), repeated with various amounts of defocus to create defocus curves, and administered a questionnaire to understand subjective, patient-reported outcomes. This study was conducted in a real-world setting and was retrospective in nature, which does not adhere to the highest standard of a prospective clinical trial. But it does allow me to give patients an idea of the outcomes they can expect, based on other patients implanted with these lenses in our clinic.
Study results
On defocus curves, all four lenses perform quite similarly to one another and much better than a monofocal or enhanced monofocal IOL. The AT-Lara lens has a slight trifocal-like defocus curve compared to the others, but overall the differences are minimal.
When we look at the distribution of patients with binocular visual acuity at various levels, all four of these IOLs produce excellent results. All patients, regardless of their intraocular lens (IOL) type, had uncorrected binocular vision of at least 0.1 LogMAR (20/25) at a distance of 400 cm and at an intermediate range of 60 cm, as well as at least 0.2 LogMAR (20/32) at a near distance of 45 cm. There are differences among the IOLs, however, particularly when we look at the percentage of patients seeing better than 0.0 LogMAR or 20/20 (Table 1). Given the small numbers in the study, the differences are not statistically significant.
Table 1: Proportion of Patients (%) with Binocular Uncorrected Acuity of 0.0 LogMAR or better
When asked about spectacle use, almost all patients, regardless of IOL type, reported using no spectacles for distance. Of course, we biased the study for perfect distance vision by only including plano patients, so this finding is not at all unexpected. The rates of spectacle use at intermediate and near distances are higher than at distance but still quite low. High percentages of patients (72% for TECNIS Symfony and AT-Lara, 84% for Vivity, and 88% for TECNIS PureSee) reported never experiencing halos, light rings, or starbursts that disturbed their vision at night. Even among those who experienced dysphotopsias, the majority did not find them particularly bothersome.
I like to look at what I call the “Never-Never-Never-Never Club” of very happy patients and the “Always-Always-Always-Always Gang” of very unhappy patients. The first group reports that they never wear glasses at any distance and never experience dysphotopsia symptoms. They are very happy because they got exactly what they wanted—spectacle independence. The second group says they have to wear glasses all the time, at all distances, and that they always experience dysphotopsia symptoms.
In this analysis, I found that while all the IRoF lenses produced satisfactory overall results, patients implanted bilaterally with the TECNIS PureSee lens were the most likely to be in the very happy group (Figure 3a) and least likely to be in the very unhappy group (Figure 3b). The difference between the TECNIS PureSee group and the other IOLs is statistically significant (p<0.5) for all the success rate comparisons and for the failure rate comparisons vs. Symfony and Vivity.
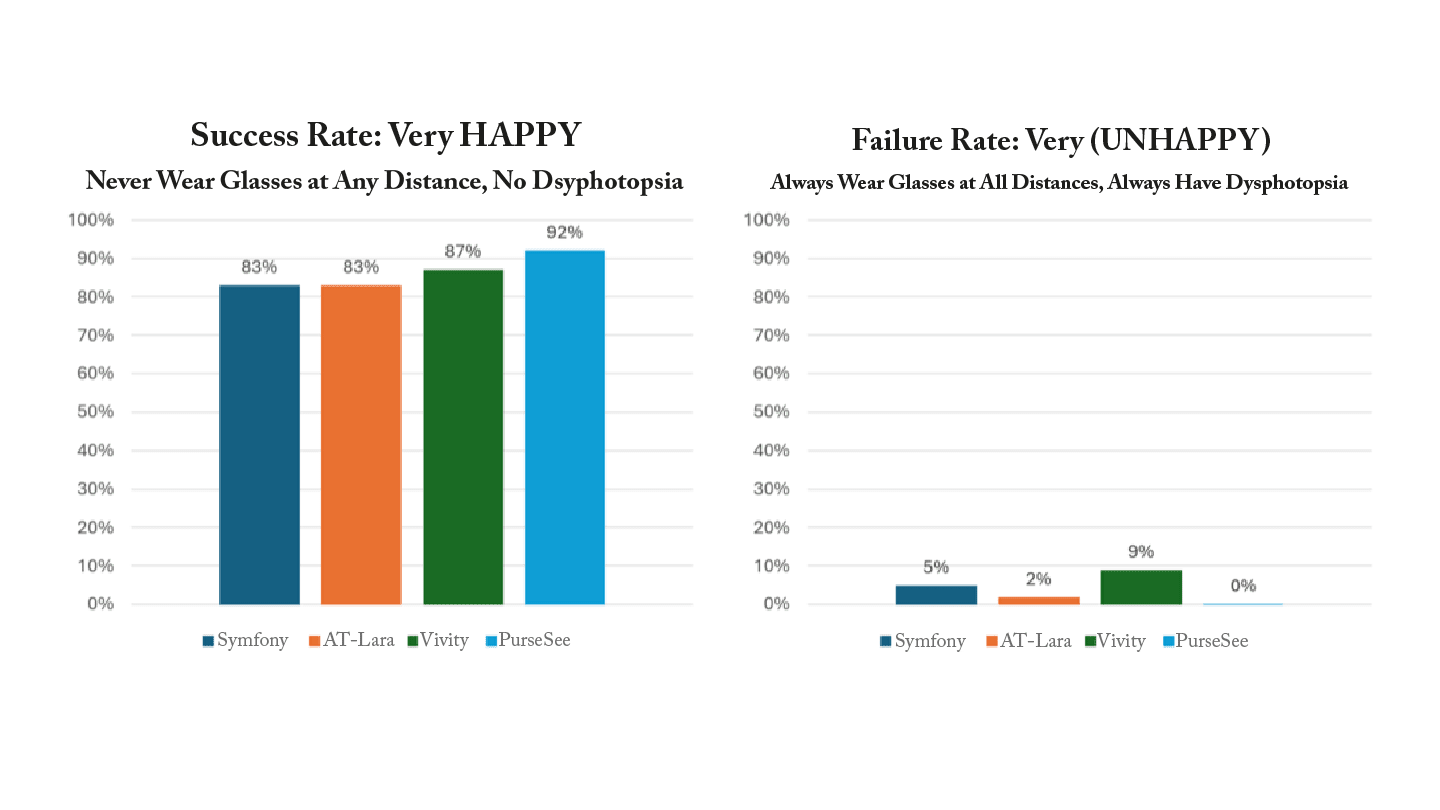
Both comparisons are important: The Never-Nevers, or ”successes,” are our biggest evangelists, telling everyone they know about the phenomenal results they achieved after surgery in our clinic. In contrast, the Always-Always Gang, referred to as the “failures,” posts terrible reviews, occupies excessive chair time, necessitates secondary procedures, and elevates surgeon stress. Fortunately, these very unhappy patients are relatively small in number, but I certainly want to minimize this group as much as possible. That is why TECNIS PureSee has become my go-to lens.
Of course, another important takeaway from this study is that biometry and astigmatism management remain critically important. If we don’t achieve near-emmetropic results, patients might not be as spectacle-independent or as happy as the patients in this study. In that case, it is not fair to blame the IOL for their dissatisfaction!
We have excellent options in the extended-depth-of-focus or IRoF category of IOLs. These lenses provide varying levels of performance related to their optical design. Interestingly, however, in this study it was not necessarily those with diffractive optics that provided more nighttime dysphotopsia, as we tend to assume. Although all IOLs tested had satisfactory success rates, the PureSee IOL seems to outperform the other lenses in terms of spectacle independence, range of vision, and reduced night dysphotopsia, making it significantly more likely that patients will be very happy with their results and less likely that they will be very unhappy compared to the other IOLs tested.
