
Standard visual field (VF) tests are based on technology that is now almost half a century old. The goal is to quantify how sensitive each part of the eye is to light, and to detect any blind spots that may indicate eye disease. First, the patient’s head is positioned on a chinrest inside a device called a “Standard Automated Perimeter” – a basin-like structure sometimes referred to with feeling as “the large toilet bowl.” Then, they are instructed to strictly fixate on a central cross, while remembering to press a button whenever they see a dot of light appear anywhere in the bowl. This procedure typically takes around 10 minutes (5 minutes per eye) – and throughout this time they must try to remain perfectly motionless from the neck up, because any head or eye movements can result in the lights appearing at the wrong location on the back of the eye: rendering the results meaningless.
Ten minutes is a long time to spent hunched in a “toilet bowl,” and it is unsurprising, then, that many people dislike the standard VF test. We know because patients told us (1). Some people are very anxious about the test, and some people fidget so much that it becomes difficult for the clinician to know whether the results can really be trusted. Furthermore, some groups of people are simply unable to perform the test – for example, young children, stroke patients, and people with cognitive impairment. We have to resort to much cruder methods to assess vision in these people. There has to be a better – meaning easier, cheaper, and more comfortable – way of assessing visual fields.
Finding a better way
Developing a new VF test, however, requires a rare mix of skills: technical expertise, clinical know-how, and experience in how to take measurements from people. On the one hand, you have to actually engineer the device: program the software and make sure that all the dots of light are precisely calibrated. But there’s also a lot of psychology involved in vision testing: for example, you need to establish if the patient is behaving in a certain way because they can’t see the lights, or because they haven’t understood the instructions, or because they are tired, or even, sometimes, because they are malingering. Constructing an automated test that controls for all of that variability is deceptively complicated. It’s easy to underestimate the challenges involved, which may be why this field has quite a high churn rate.
Fortunately, when developing our new system, we had access to a great team of people: the lab is run by David Crabb, who has been working on ways to improve vision testing for many years, and the project has benefited tremendously from the clinical insights of consultant Daniel Lindfield. Moreover, we have had wonderful support from all the staff and patients at the Royal Surrey County Hospital.
The basic idea behind our approach is very simple – like the standard test, our device – Eyecatcher – presents lights to different parts of the eye, and the patient responds when they see them. But our technology differs from standard systems in three important ways.
First, patients no longer need to press a button. Instead, they simply need to look towards any lights that they notice – a natural reflex which is present pretty much from birth (2). Eyecatcher then uses an eye-tracker (basically a little camera below the screen) to automatically determine whether or not the patient responded correctly. Relying on the eye’s normal reaction means that we don’t have to give patients any complex instructions; we just put them in front of the device and leave them to respond naturally. And this also removes some of the measurement variability, since you’re less likely to “forget” to respond, or to look in exactly the right location by chance.
Second, we’re able to remove altogether the uncomfortable chinrest and central fixation cross. In the standard test, those things are really important for making sure the lights are projected onto exactly the right part of your eye. However, Eyecatcher doesn’t really care if you move your head or your eyes, since we can use the camera to measure exactly what you’re doing. If you move forwards, the spot automatically gets smaller, if you move backwards, the spot of light gets bigger, so it’s always the right size even if you move your head. Similarly, wherever you happen to be currently looking, we can choose to present points to the left or to the right (etc.), so the light always appears at the right location in your eye. Essentially, the idea is that Eyecatcher does all the hard work, rather than the patient. This makes the test more comfortable, and means we don’t have to rely on the patient being “well-behaved” in order to get good data.
Third, we’ve replaced the hated toilet bowl with an ordinary computer screen (Figure 1). At present, we’re using a portable tablet computer display the stimuli, but the program can run equally well with a monitor or a TV screen. This doesn’t necessarily make the results of the assessment any better, but means that our approach is user-friendly, versatile, and really cheap to setup and maintain.
Glaucoma case-finding with Eyecatcher: feasibility study
The combination of an inexpensive eye-tracker and a portable tablet computer enables visual field assessment without the need of head restraints or button-pressing; the device infers stimulus detection from changes in the direction of gaze. But can Eyecatcher actually identify glaucoma cases? Results from a pilot study are very encouraging (3).
- Subjects: 12 glaucoma patients (24 eyes), six age-similar controls (12 eyes)
- Method: Test once per eye with both Eyecatcher and standard automated perimeter (HFA SITA standard 24-2)
- Eyecatcher: subject instructed to look at a sequence of fixed luminance dots presented relative to the current point of fixation; start and end fixations identify locations where stimuli are seen / unseen; gives continuous map of sensitivity loss across VF of ~20 degrees
- Standard automated perimeter: normal method was followed
- Results:
- Eyecatcher clearly separated patients from controls and gave results consistent with standard automated perimetry
- Mean Eyecatcher scores were strongly correlated with mean deviation scores from the standard device: p<0.001
- Eyecatcher and standard device showed 84 percent concordance between corresponding VF locations
- Participants reported that Eyecatcher was more enjoyable, easier to perform, and less tiring than the standard system (all p<0.001)
- Conclusion: Portable perimetry with an inexpensive eyetracker / portable tablet computer is feasible and could be the basis of a new system to rapidly and cost-effectively screen patients.
Where now?
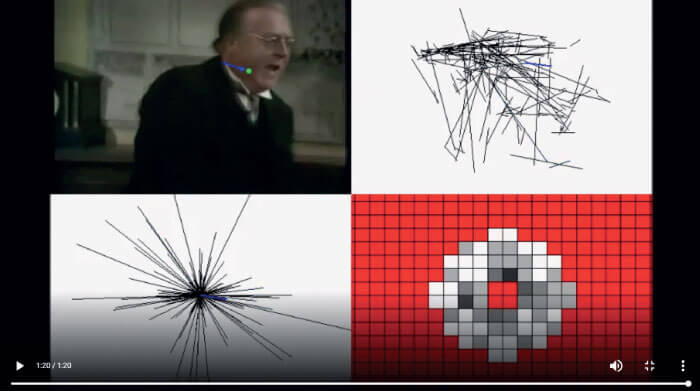
There are still a few kinks to be ironed out with the eye-tracking component of Eyecatcher. Even really good eye-trackers can struggle to track “unusual” eyes, including those with heavy make-up, or those that have recently undergone surgery. Fortunately, many companies full of much cleverer people than us are working to develop the basic hardware; there have been immense improvements already over the last five years, and systems are only going to get better, cheaper, and smaller with time. Indeed, from a technology perspective, the possibilities are almost limitless. For instance, one of our PhD students, Daniel Asfaw, is exploring whether we can get rid of flashing lights altogether (5) – the idea is to simply run the test while the patient watches TV (Figure 2).
The real challenge, however, will be to translate the device from lab to real life. Going from proof-of-concept to something that has a significant clinical impact is a huge step, and will require involvement of many different stakeholders: patients, clinicians, investors. Our one big advantage is that we’re not personally looking to make money. We’ve been really fortunate to be funded by the eye charity Fight for Sight (UK), and that means that we’re free to work with anyone – from large organizations to individual clinicians – who may be interested in using, adapting, or improving Eyecatcher.
Possible applications
In the first instance we’re not looking to provide a like-for-like replacement for existing tests. Our main vision for Eyecatcher is for it to be used as a rapid triage device. Glaucoma clinics are currently under colossal strain; partly due to aging populations, but mainly because they’re increasingly being sent people who have been referred “just in case," but who in truth have healthy eyes and don’t need to be there. Eyecatcher could help to quickly and cheaply weed some of these cases out, and so help relieve the increasing pressure on glaucoma clinics
Furthermore, the equipment is so cheap that we’re considering whether we could just give it to people to take home. This would enable patients to regularly and conveniently test themselves, and might thereby help to pick up any sudden progression in their symptoms, rather than having to wait six to twelve months for a regular hospital appointment – during which time they may suffer irreversible sight loss. This is something we’re exploring with our colleagues Tamsin Callaghan, Peter Campbell and David Edgar, and we have recently received funds from the International Glaucoma Association to give 20 people the chance to use Eyecatcher at home for a year. This is a really interesting trial – we just don’t know what will happen. Maybe people won’t use it properly; maybe they’ll stick it a drawer and not use it at all; or maybe it will work brilliantly! This is a big issue, as there’s huge interest right across healthcare in the idea of home-monitoring: the potential gains in convenience and cost-savings alone are huge, but we just don’t know if it really works in practice.
Finally, a low-cost, portable VF test such as Eyecatcher could be great for taking out into communities that have difficulty accessing eye care. It could be particularly useful in developing countries, such as those in Sub-Saharan Africa with sparse, rural populations, and relatively few local eye-care services. For those people, getting to an eye care professional is not always an option, and bring the existing VF tests to them is hardly practicable, considering you’re talking about a device the size of a washing machine, that requires a reliable power source such as a diesel generator. A low-cost, solar-powered tablet-test could make an enormous difference to these countries, many of which have even higher incidence rates of glaucoma than the UK. To this end, we are working with colleagues at the London School of Hygiene and Tropical Medicine and Peek Vision (6) to explore Eyecatcher’s potential as a cheap case-finding device in rural regions and developing countries.
Last words
With Eyecatcher, we can examine someone’s VF while allowing patients to do what comes naturally to them – move their eyes. They don’t need detailed instructions – all that’s required is to sit in front of a screen and behave normally. And thanks to all the fantastic new technologies that are now available – tablets, smartphones, eye-trackers, and so-on – we’ve been able to construct a test that is quick, cheap, portable, and comfortable. We’re very optimistic about its potential: initial data suggest that it gives results comparable to those from more established devices, and the feedback indicates that patients actually like doing it. And it’s particularly encouraging that we’re not alone in noticing the potential benefits of all these new “disruptive” technologies. There are groups right across the world – in Singapore, Australia, and Scotland – all trying to develop similar devices, and that has to be good for patients in the long run. The VF testing field has lain fallow for too long, and I’m delighted that it’s finally being revisited.
Clinician’s View
Consultant ophthalmologist Dan Lindfield can see first-hand how important portable visual field-testing options are for glaucoma patients:
Visual field testing remains vital in the management and diagnosis of glaucoma. It is the only method we have for seeing what our patients can see. However, in recent years devices measuring optic disc structure have received heavy investment and made huge leaps forward, while devices measuring function have been relatively dormant. Static perimetry has evolved and remains the gold standard for disease monitoring but the learning curve and patient difficulties often stifle its use in case finding and diagnosis. The mismatch of machine location to disease location is also a major factor in our hunt for patients with glaucoma. Low-cost, portable eye tracking technology has the potential to revolutionize access to potential cases of glaucoma not just in the developing world, but also in our local towns and cities. It may remove the hurdle of patients needing to attend an eye professional, and “background” home testing while we watch TV is only a small step forward from where we are. We live in exciting times for visual field testing. It is time to bring it out from a dark room.
Find out more about The Crabb Lab at http://www.staff.city.ac.uk/crabblab/#/ and follow its developments on Twitter @crabblab.
References
- FC Glen et al., “A qualitative investigation into patients’ views on visual field testing for glaucoma monitoring”, BMJ Open, 10 (2014). PMID: 24413347. PR Jones et al., “Automated measurement of resolution acuity in infants using remote eye-tracking”, Invest Ophthalmol Vis Sci, 55, 8102-8110 (2014). PMID: 25352118. PR Jones et al., “Portable perimetry using eye-tracking on a tablet computer – a feasibility assessment”, Transl Vis Sci Technol, 8 (2019). PMID: 30740267. D Crabb et al., “What's on TV? Detecting age-related neurodegenerative eye disease using eye movement scanpaths”, Front Aging Neurosci, 6m 312. https://doi.org/10.3389/fnagi.2014.00312. PMID: 30740267. DS Asfaw et al., “Does glaucoma alter eye movements when viewing images of natural sciences? A between-eye study”, Invest Ophthalmol Vis Sci, 59, 3189 (2018). PMID: 29971443. Peek Vision (2019). Available at www.peekvision.org. Accessed May 14, 2019.
