When most healthcare workers hear the word “ophthalmology,” they quite appropriately think about pathology that occurs in the eye rather than near the eye. A more encompassing metric is to consider the eye an extension of the brain and a critical structure making up the skull base.
To exemplify the need for this critical distinction, consider the following case: a 65-year-old patient was referred to Wills Eye Hospital from Arizona with a 14-month history of progressive facial problems.
His symptoms started with numbness of the right side of his forehead, developing over several months to a facial palsy and double vision. He was eventually sent to us because his right eye had progressively worsening motility.
Multiple MRIs performed locally were read as normal. He was evaluated by the Neuro-Ophthalmology Service and was found to have multiple cranial nerve abnormalities and severe restriction of the movement of the right eye. A detailed past medical history was not contributory. So, what should we do now?
At Wills, we have ophthalmologic sub-specialists that can manage any ocular problem. We’re also extremely fortunate to be affiliated with Thomas Jefferson University Hospital (TJUH) and a group of neurosurgeons, otolaryngologists, neuroradiologists, oncologists, and radiation therapists that are second to none.
Over several decades, I’ve had the privilege of working closely with these professionals and we have established a collaborative skull base team that has managed complex cases from the entire country and abroad.
The skull base is an anatomic confluence of the base of the brain, the orbits, and the paranasal sinuses. It’s densely packed with critical structures, including the internal carotid arteries, the optic nerves, the venous sinuses, and cranial nerves that travel through the various “nooks and crannies” that connect the orbits to the intracranial vault.
The skull base is also the confluence of multiple surgical specialties; successful patient management requires a complex interplay between orbital surgery, neurosurgery, and otolaryngology, which may not be available at many institutions.
Furthermore, technologic advances in neuroradiology, intraoperative image guidance, cerebral angiography, and trans-nasal endoscopic techniques have allowed for minimally invasive surgical management. Our otolaryngologists, neurosurgeons, and orbital surgeons can access the orbital apex, pituitary fossa, and clivus through the nose.
Our neurovascular team can snake a catheter into an infant’s ophthalmic artery to directly treat retinoblastoma with chemotherapy, or close a carotid-cavernous fistula through the superior ophthalmic vein via a lid crease incision. And if a combined tumor resection is needed, the microvascular free flap team can safely close large defects across the orbit, face, and skull.
Such cases are not easy. They require a trust and collaboration between surgeons that is built over many years and many procedures – and that’s what we’ve achieved here at Wills and TJUH. Each surgical specialty learns from the other and, consequently, patients benefit.
It’s been a long road to get to where we are – a lot of long hours, sleepless nights of worry, and days of inpatient rounding. Some cases are less successful than we initially hoped for, but patients quickly realize that they are in a center with experience and dedication: our physicians try their best in every single case.
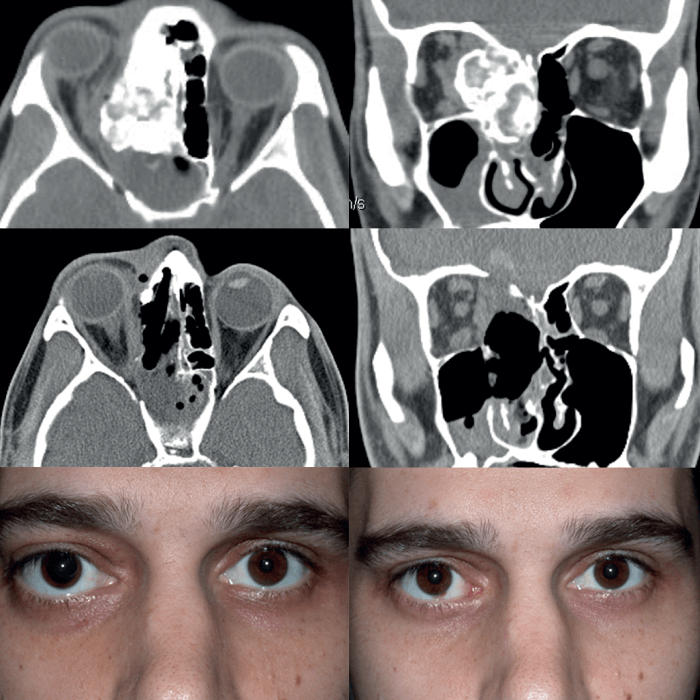
So, what happened to our patient from Arizona? A skull base MRI was obtained and the patient was seen by orbital surgery and neurosurgery, all on the same day. Review of all previous MRIs by our neuroradiologists revealed that there was in fact a process along the supraorbital nerve (the sensory nerve that supplies the forehead) that had progressed over many months and had now extended into the cavernous sinus.
The patient was noted to have sun damaged skin across his entire face, but denied any history of skin cancer. However, on more detailed questioning, he recalled that his dermatologist had been “freezing and burning things off my forehead for years.”
A skull base biopsy was performed and confirmed our suspicions – the patient had an undiagnosed squamous cell carcinoma from his forehead skin that had invaded his supraorbital nerve and crept back into the cavernous sinus, infiltrating multiple other nerves in the skull base. The case was discussed at the Head and Neck Tumor Board and radiation and chemotherapy were recommended.
It’s been a privilege to work with my colleagues at TJUH – their technical expertise is humbling and their dedication is inspirational. And it’s just one of the many puzzle pieces that makes Wills a great place to be – for both patients and physicians.
