Initial outcomes with the IC-8 IOL are clearly good – but what are the longer-term implications of a small aperture IOL? Does it hinder taking refraction, interfere with retinal visualization or impede subsequent retinal surgery? Certainly, some procedures need minor adjustment: Beltz points out that, due to the increased depth of focus, it can be difficult to determine a suitable “end point” while refracting. “The best method to use is termed ‘mid-point refraction’ and involves performing a normal manifest refraction and then establishing the maximum plus lenses to blur and the maximum minus lenses to blur – then you calculate the mid-point.” Beltz notes that it is also acceptable to perform a red/green balance test. Shiu concurs: “We usually use the red and green method to ensure we are not giving patients extra refraction due to the extended range of vision.” Vote states that autorefractors do not perform well in eyes that have been implanted with an IC-8 IOL: “Consequently, refractive outcomes should be assessed subjectively.”
Regarding subsequent surgery, Ham has this comment: “In a dilated pupil, we can view the retina fairly well so I think retinal surgery in an IC-8 IOL eye will be
reasonably straightforward. There may be exceptions depending on the VR surgeon.” – Vote too does not anticipate significant issues: “Modern VR operating systems (such as BIOM) deal very well with small pupils.” Chan reminds us of a UK report (1) indicating that the IC-8 IOL does not impede the intra-operative view during pars plana vitrectomy, and Auffarth notes anecdotal reports from German surgeons that retinal detachment and peeling surgery can be performed in IC-8 IOL eyes. Srinivasan concurs: “There is no issue regarding performance of retinal surgery in IC-8 IOL eyes. I have personally assisted a retina colleague on an IC-8 IOL eye where the surgeon noted the lens did not impede viewing of the posterior segment or his ability to perform pars plana vitrectomy.” Srinivasan also noted: “The advantage the IC-8 IOL has is the center and periphery of the lens is a monofocal optic so the retinal surgeon does not have to constantly change focus of the microscope like when working through refractive and diffractive rings.”
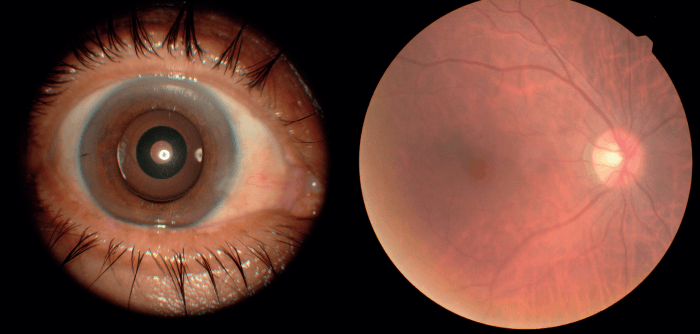
"In IC-8 IOL eyes we can perform all routine retinal examinations including OCT without concern for image quality." Sathish Srinivasan
Fundus Photography in an Eye Implanted with IC-8 IOL. Photo Courtesy of Gabriel Quesada, MD.
How does one deal with PCO in an IC-8 IOL implanted eye? Vote puts the issue in perspective: “All IOLs designed to give spectacle independence are sensitive to PCO.” He asserts, however, that YAG can be performed through the IC-8 IOL aperture: “Take care not to hit the mask with the laser – you won’t affect quality of vision but you may change the visual appearance of the IOL, with cosmetic consequences.” Alternatively, Vote says, we can go around the outer edge of the mask, gaining access via a U-shaped flap hinged at the bottom: “I find this approach provides more lasting benefits.” Chan agrees: “My personal preference is to perform laser outside the mask, as this allows a better view of the fundus when the pupil is dilated.” Shiu also prefers to apply YAG from outside the periphery; his experience is that this procedure restores patients’ vision very quickly. By contrast, Beltz prefers to apply laser through the central aperture. Srinivasan takes the view that neither technique (through-the-middle versus around-the-edge) is better than the other: “Both are good – which one you use depends on how the capsule falls.”
With regard to performance in dim light conditions, Vote states that although patients may be aware of a difference between the eyes if they cover each eye in turn, the awareness will diminish over time and in any case is insignificant: “In our visual system, the pupil only accounts for one log unit of the total 10-11 log units of light adaptation.” Chan notes that he has had few complaints of patients experiencing difficulty under low light conditions; nevertheless, he warns patients that they may need glasses to read in dim light. He adds: “Research indicates that perceived brightness with the IC-8 IOL is higher than predicted by simple calculation of actual light reaching the retina through the central aperture.”(2) Shiu emphasizes monolateral IC-8 IOL recipients will have enough light in the dominant eye for neuroadaptation to provide good bilateral low-light vision. He also notes the importance of expectation management: “We tell patients they will need reading glasses in some circumstances – and because there are no surprises, we get few complaints.” Auffarth and Srinivasan state that none of their patients has reported significant night vision difficulties; similarly, Beltz reports that her patients have very high satisfaction with vision in dim light: “The mean satisfaction scores for dim light and bright light vision were equivalent.”
“The IC-8 IOL is an important alternative to diffractive IOLs, as it is not associated with halo or glare issues in my experience.” Gerd Auffarth
Could the IC-8 IOL small central aperture affect the ability to examine the retina? Vote thinks not: “The mask only extends to 3.23 mm in total, and the peripheral IOL remains clear – peripheral retinal details can be seen easily.” He adds that OCT is not typically impacted. Chan agrees: “There is no problem performing OCT or OCT angiography through an IC-8 lens.” He further notes that fundus examination is also little affected by the small aperture, although it is more difficult if the pupil is not dilated. Auffarth agrees: “For the experienced ophthalmologist, retinal examination in IC-8 IOL eyes will not be a big issue.” Beltz is unequivocal: “I have not had any issues with fundoscopy or OCT imaging; no special attachments or variations to technique are required to image the retina with the IC-8 IOL in place.” She goes on to cite Srinivasan’s data from 10 patients (1): “These showed that standard posterior segment investigations including non-mydriatic fundus photography, optical coherence tomography, and automated perimetry could be safely and effectively performed in eyes with small aperture IOLs.” She adds that the data did not indicate differences in quality between images taken from small and standard aperture IOLs. Srinivasan corroborates this: “In IC-8 IOL eyes we can perform all routine retinal examinations including OCT without concern for image quality.”
View the next article in the series
To view all parts of this series, go to The IC-8 IOL: Big Advantages Through Small Apertures
To download the full publication, please click here
Go to the next part, Expert Consensus on the IC-8 IOL

To see the other parts of this series, go to The IC-8 IOL: Big Advantages Through Small Apertures
To download the full publication, please click here
References
- S Srinivasan et al., “Posterior segment visualisation in eyes with small aperture IOL”, J Refract Surg, 35, 538-542 (2019) PMID: 31393993.
- S Manzanera et al., “Adaptation to brightness perception in patients implanted with a small aperture”, Am J Ophthalmol, 197, 36 (2019). PMID 30236772.
