Stevens-Johnson syndrome (SJS) and toxic epidermal necrolysis (TEN) are severe and potentially lethal multisystem, mucocutaneous, immune-mediated adverse drug reactions (IM-ADR). These related conditions are as rare as they are serious, with an incidence of about 1 to 7 cases per million per year and an overall mortality rate of 20–25 percent (1, 2). Medications trigger SJS/TEN in greater than 80 percent of the adults who are diagnosed with it, and the onset typically occurs within a few weeks of administration of the culprit drug (3, 4). Antibiotics and anticonvulsants are among the most commonly implicated triggers.
Ocular involvement is associated with the vast majority of these cases. In fact, progressive conjunctival scarring and corneal damage are the most disabling long-term complications for SJS/TEN survivors (5). Secondary systemic complications often seen with SJS/TEN include dermatologic, respiratory, genitourinary, and psychiatric disorders, including post-traumatic stress disorder. Due to the unusual nature of the disease, practicing ophthalmologists will rarely, if ever, see a case. However, it is imperative to understand the pathology and recognize symptoms so that a swift referral can be made to an ICU or dedicated burn unit in order to give these patients their best chance at a successful outcome.
Diagnosis and referral
The management of SJS/TEN-associated ocular sequelae is extremely challenging. Because these conditions are so rare, the comprehensive ophthalmologist tends to be unfamiliar with the presenting signs of the disease, its acute management, and long-term consequences. There is a short window of opportunity during the acute stage when intervention may potentially avoid lifelong complications, which may include photophobia, intractable dry eye, chronic pain, corneal scarring, and severe vision loss – all of which are associated with diminished quality of life. And that’s why education is a major aim among those of us who are actively involved in SJS/TEN research and treatment.
Suspecting a diagnosis, immediately referring the patient to a regional burn center, and identifying the culprit drug are all critical to optimal management. The clinical presentation usually starts with a prodrome of fever, malaise, cough, rhinorrhea, and anorexia followed by mucositis and a painful generalized erythematous vesiculobullous rash with skin sloughing (6, 7). Early signs of ocular disease can be variable, ranging from conjunctival hyperemia to sloughing of the entire ocular surface and eyelid margin epithelium.
Underscoring my point about education: up to one-third of cases may be misdiagnosed, which also highlights the importance of gaining histological confirmation from a skin biopsy at the outset of the rash (8).
There is a well described genetic and ethnic predisposition to SJS/TEN. A significantly strong correlation was first found with the Han Chinese population in 2004. Carbamazepine (CBZ) induced SJS/TEN patients carried 100 percent of the HLA-B*1502 allele, and only 3 percent of HLA-B*1502 carriers tolerated CBZ. Based on its absence in Caucasian and the Japanese, the HLA-B*1502 allele seems uniquely limited to Han Chinese ancestral Asians and might be an explanation for the extremely high risk of CBZ-induced SJS/TEN in Southeast Asians compared with Caucasians and the Japanese (9). This knowledge has not only led to successful HLA-B*1502 screening programs in Taiwan, Singapore, and other parts of Southeast Asia (which have almost eliminated CBZ-associated SJS/TEN), but also furthered our understanding of the immunopathogenesis of SJS/TEN (10). Recent studies show that a network of susceptibility genes for SJS/TEN, such as TLR3, EP3, and IKZF1, may trigger the inflammation associated with several ocular complications (11, 12).
Ocular involvement
SJS/TEN can be divided into acute and chronic phases. The acute ocular symptoms manifest as inflammation of the entire ocular surface: cornea, bulbar and tarsal conjunctiva, and eyelid margin. This process runs the gamut from mild conjunctival injection to severe pseudomembranous conjunctivitis, corneal epithelial dysfunction, melting and perforation, and eyelid margin scarring. If inflammation persists, it may result in the chronic manifestations of the disease, such as symblepharon formation and forniceal shortening. In addition to the conjunctival inflammation, there may be damage of the mucin-producing goblet cells, lacrimal ducts, and meibomian glands, as well as keratinization of the ocular surface (6, 13). The most important prognostic factor in long-term outcomes of SJS/TEN is keratinization and scarring of the eyelid margins (14, 15). Other lid margin abnormalities that may develop include entropion, trichiasis, and punctal occlusion.
Patient management
Loyola University in Chicago, Illinois, USA, is the referral center for SJS/TEN cases that arise throughout the Chicagoland area. We have been the go-to establishment for 25 years, due, in large part, to the work of Richard Gamelli, who established the main burn unit that is the hub of five similar units throughout the city. When patients are suspected of having SJS, they are sent directly to our burn unit. Though most ophthalmologists may see one SJS/TEN patient at the most throughout their career, we see 8–12 of these patients every year (16).
Because of the multisystem nature of the disease and the high mortality rate, patients with SJS/TEN should be managed in the ICU or dedicated burn units that have the capabilities to provide complex skin care and appropriate intensive care for more severe cases. This approach has been shown to improve outcomes (17). Stopping the culprit drug is also associated with a better prognosis for these patients; however, identification of the causal drug can be extremely challenging and often relies mainly on expert judgment – but every day of delay worsens the outcome (18).
Because of the frequent involvement of the eye in SJS/TEN, ophthalmologists need to be involved as early as possible. An initial ocular examination on all SJS/TEN patients should occur within 24 to 48 hours of admission. Unfortunately, patients don’t always have the benefit of an ophthalmologist’s input early in the process. In fact, only 66 percent of burn ICUs in the US consult ophthalmology for SJS/TEN patients (8, 13). Ocular involvement can be severe very early in the disease, even before extensive skin sloughing has occurred. Traditionally, the first two to six weeks following onset of symptoms is recognized as the acute stage. But ocular involvement in SJS/TEN can be fluid; a case that is moderate one day may become severe the next, making daily examinations crucial in the acute phase.
Ocular surface damage often represents the most significant long-term complication of SJS/TEN. It has been reported that a majority of patients with late ocular complications find it difficult to read, drive at night, and use a computer for several hours at a time. The chronic ocular complications of SJS/TEN are caused by prolonged ulceration and ongoing inflammation that leads to scarring of the ocular surface. A major underlying cause of sight-threatening corneal complications is the continuous trauma caused by friction from the scarred mucosal surfaces of the eyelids. Even when patients do not lose vision, scarring in the fornix disrupts lacrimal gland function and causes dry eye syndrome – the most common complication.
Treatment evolution
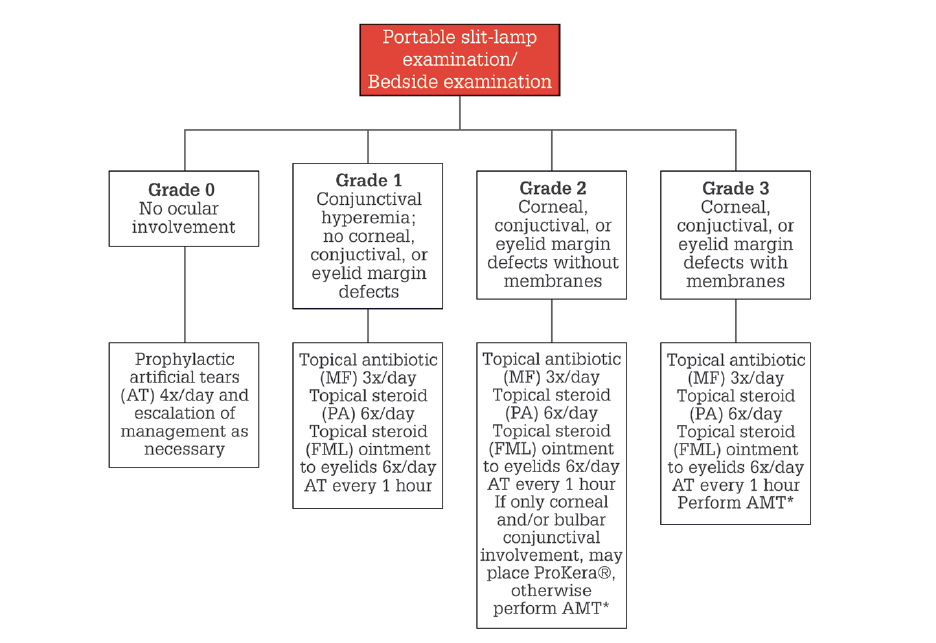
The treatment of acute SJS/TEN involves a grading system of ocular severity (see Figure 1).
For Grades 0 and 1, daily saline (NaCl 0.9%) flushes should be performed and pseudomembranes debrided with a cotton-tipped applicator. Medical treatment should include moxifloxacin 0.5% drops (Vigamox) three times a day, topical steroid eye drops six times a day, and a steroid or antibiotic-steroid combination ointment to the eyelid margins four to six times a day. Cyclosporine 0.09% drops (Cequa, Sun Pharma) four times a day should also be considered. Preservative-free artificial tears should be used every one to three hours in between the other drops.
For grades 2 and 3, amniotic membrane transplant (AMT) is at the forefront of SJS/TEN management. This should be done within seven days of the onset of the skin rash, in cases with significant eyelid margin involvement +/– bulbar conjunctiva (see Figure 2) (19, 20). Systemic management is controversial, though drugs such as etanercept (a TNF-α receptor antagonist) and cyclosporine (an immunosuppressant) are showing promise in ongoing clinical trials, including one in which Loyola is a participant. Pulse systemic corticosteroid has been used in Japan since 2005 with beneficial results.
Amniotic membrane transplant (AMT)
Amniotic membrane (AM) tissue has played a vital role in treatment of a variety of ocular surface conditions since 1940, when de Rött first reported on the use of fresh amnion and chorion as a biological dressing material for management of conjunctival defects (21). More recently, in 2002, John and colleagues reported the first use of AM in acute SJS (22).
Currently, there are two types of amniotic membrane tissue: dehydrated and cryopreserved. Cryopreserved AM (CAM) promotes regenerative wound-healing (23, 24, 25). The cryopreservation process allows CAM to retain key properties (heavy chain peptide [HC], hyaluronic acid [HA], pentraxin-3 [PTX3]) that are lost in the dehydration process. These biologic compounds are responsible for CAM’s anti-inflammatory and regenerative healing properties, such as tissue repair and remodeling (23, 24, 25, 26).
Early work with AM grafts for SJS/TEN focused on coverage of the entire ocular surface where both the ocular surface and the lid margins must be covered with AM to inhibit inflammation, scarring, and vision loss (22). A self-retained contact lens-like CAM device, known as Prokera (BioTissue), has also been used for isolated corneal epithelial defects without significant lid margin involvement (6, 7). BioTissue is currently the only company associated with cryopreserved AM.
To effectively perform AMT for SJS/TENS patients in the vast majority of cases, we need a large enough piece of tissue to cover the upper eyelids and to coat and cover the internal surface on the inside — specifically, the upper part of the eyelid and the inside of the lower eyelid. This need is what makes cryopreserved AmnioGraft (BioTissue) indispensable to the process. There are no other AM tissue products available that are large enough to effectively cover all the territory required to manage severe acute ocular manifestations of SJS/TEN.
A major development that has taken AMT grafts to the next level in the SJS/TEN treatment hierarchy is the ability to perform the AmnioGraft procedure with cyanoacrylate glue instead of sutures. This obviates the need to send these very sick patients to the operating room. Instead, when we secure the AM to the upper and lower eyelids with glue it can be done at the bedside (27, 28). The procedure that we use today is similar to the one described by Shanbhag and colleagues (28).
The AMT procedure
In the acute SJS/TEN patient with moderate-to-severe ocular disease involving the eyelid margin, cornea, and/or conjunctiva, a continuous 5 cm x 10 cm sheet of cryopreserved AM is separated from the nitrocellulose paper at one edge and draped over the eyelid margins in a vertical orientation with the epithelial basement membrane side up. The tissue can be secured with a running suture along the upper and lower eyelids or secured to the lid margins with cyanoacrylate glue (Ethicon).
Cyanoacrylate glue is placed underneath the AM on the upper eyelid margin skin, several millimeters away from the eyelid margin. The AM is then held across the upper eyelid for 30 seconds with 2 forceps to ensure adhesion. A Desmarres retractor is used to lift the upper eyelid off the ocular surface, and a custom symblepharon ring is used to push the AM into the superior fornix and then the inferior fornix. This is done carefully to ensure the AM remains flat and unwrinkled under the symblepharon ring. A muscle hook is used to flatten and spread the AM into the desired position, and cyanoacrylate glue is then placed on the skin of the lower eyelid several millimeters away from the eyelid margin, and the AM is draped over the glue. Excess AM beyond that which is attached to the eyelid margins is trimmed with scissors. Antibiotic ointment is applied over the eyelid and ocular surface, and the sterile drape is removed. At this point, the surgeon should ensure that the patient is able to close the eyelid and that there is no lagophthalmos secondary to the symblepharon ring.
Treatment challenges
The biggest challenge inherent in the use of AM for SJS/TEN treatment is that the procedure must be started within a week of the onset of the skin rash. If a patient undergoes AMT weeks later, the treatment is not as effective. Long-term results show that early use of AM in the acute phase of SJS/TEN is effective in mitigating severe vision loss (29). Despite a growing body of evidence describing early AMT as a means of preventing serious long-term sequelae, many patients still go untreated and thereafter experience severe photophobia, painful dry eye problems, and blinding cicatricial ocular surface complications indefinitely. The sooner AMT is performed, the more effectively it can prevent scarring sequelae. The window of opportunity begins to close after the onset of ocular surface sloughing. After this acute period, intractable scarring sets in.
Resolution of the epithelial defects on the ocular surface reflects a favorable outcome. For more severe disease, multiple grafts may be necessary over a 2–4-week period. For chronic disease, multiple treatments have been reported to be effective in the management of ocular surface scarring, including Scleral PROSE contact lenses and mucus membrane grafting (MMG) for lid margin keratization (30, 31). Timely MMG can significantly alter the course of disease and not only preserve but improve vision in affected eyes (32). In one study, patients receiving suboptimal care during acute SJS presented later with severe ocular and visual morbidity; two-thirds of patients (99 percent without prior amniotic membrane grafting) presented more than a year after acute SJS with low vision or blindness in 60 percent of eyes (33).
Keratoprosthesis (KPro) is probably the optimal surgical intervention for visual rehabilitation in end-stage ocular SJS/TEN. It can restore fairly good visual function; however, it is associated with complications and the need for repeat procedures (34). Patients with SJS/TEN tend to experience device retention and have more severe post-operative complications and a poorer visual prognosis relative to other indications.
Takehome
SJS and TEN are rare multisystem allergic drug reactions with significant ocular sequelae if left untreated within a narrow window of time using amniotic membrane grafting. Early recognition, diagnosis, and referral of SJS/TEN patients to a burn unit or ICU offers the patient the best chance for a favorable outcome.
References
- R Hazin et al., “Stevens-Johnson syndrome: pathogenesis, diagnosis, and management,” Ann Med, 40, 129 (2008). PMID: 18293143.
- J Schneck et al., “Effects of treatments on the mortality of Stevens-Johnson syndrome and toxic epidermal necrolysis: A retrospective study on patients included in the prospective EuroSCAR Study,” J Am Acad Dermatol, 58, 33 (2008). PMID: 17919775.
- AM Oakley AM, K Krishnamurthy, Stevens Johnson Syndrome. StatPearls Publishing: 2020.
- MA Miliszewski et al., “Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis: An analysis of triggers and implications for improving prevention,” Am J Med, 129, 1221 (2016). PMID: 27086495.
- HY Lee et al., “Long-term complications of Stevens-Johnson syndrome/toxic epidermal necrolysis (SJS/TEN): the spectrum of chronic problems in patients who survive an episode of SJS/TEN necessitates multidisciplinary follow-up,” Br J Dermatol, 177, 924 (2017). PMID: 28144971.
- S Kohanim S et al., “Acute and chronic ophthalmic involvement in Stevens-Johnson Syndrome/Toxic Epidermal Necrolysis - A comprehensive review and guide to therapy. II. Ophthalmic Disease,” Ocul Surf, 14, 168 (2016). PMID: 26882981.
- HN Saeed, J Chodosh, “Ocular manifestations of Stevens-Johnson syndrome and their management,” 27, 522 (2016). PMID: 27585215.
- HG Le et al., “Burn unit care of Stevens Johnson syndrome/toxic epidermal necrolysis: A survey,” Burns, 42, 830 (2016). PMID: 26810444.
- KD White et al., “SJS/TEN 2017: Building multidisciplinary networks to drive science and translation,” J Allergy Clin Immunol Pract, 6, 38 (2018). PMID: 29310768.
- KD White et al., “Evolving models of the immunopathogenesis of T cell-mediated drug allergy: The role of host, pathogens, and drug response,” J Allergy Clin Immunol, 136, 219 (2015). PMID: 26254049.
- M Ueta et al., “Trans-ethnic study confirmed independent associations of HLA-A*02:06 and HLA-B*44:03 with cold medicine-related Stevens-Johnson syndrome with severe ocular surface complications,” Sci Rep, 7, 5981 (2014). PMID: 25099678.
- CC Lin et al., “Stevens-Johnson syndrome and toxic epidermal necrolysis: risk factors, causality assessment and potential prevention strategies,” Expert Rev Clin Immunol, 16, 373 (2020). PMID: 32154748.
- SS Shanbhag et al., “Long-term effect of a treatment protocol for acute ocular involvement in Stevens-Johnson Syndrome/Toxic Epidermal Necrolysis,” Am J Ophthalmol, 208, 331 (2019). PMID: 31326519.
- MA Di Pascuale MA et al., “Correlation of corneal complications with eyelid cicatricial pathologies in patients with Stevens-Johnson syndrome and toxic epidermal necrolysis syndrome,” Ophthalmology, 112, 904 (2005). PMID: 15878074.
- C Sotozono et al., “Predictive factors associated with acute ocular involvement in Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis,” Am J Ophthalmol, 160, 228 (2015). PMID: 25979679.
- PD Bustros et al., “Review of culprit drugs associated with patients admitted to the Loyola University Medical Center Burn Unit with the Diagnosis of Stevens-Johnson Syndrome,” Burns (2021).
- VM Lim et al., “A decade of burn unit experience with Stevens-Johnson Syndrome/Toxic Epidermal Necrolysis: Clinical pathological diagnosis and risk factor awareness,” Burns, 42, 836 (2016). PMID: 26847613.
- I Garcia-Doval et al., “Toxic epidermal necrolysis and Stevens-Johnson syndrome: does early withdrawal of causative drugs decrease the risk of death?” Arch Dermatol, 136, 323 (2000). PMID: 10724193.
- DG Gregory, “Treatment of acute Stevens-Johnson syndrome and toxic epidermal necrolysis using amniotic membrane: a review of 10 consecutive cases,” Ophthalmology, 118, 908 (2011). PMID: 21440941.
- DG Gregory, “New grading system and treatment guidelines for the acute ocular manifestations of Stevens-Johnson Syndrome,” Ophthalmology, 123, 1653 (2016). PMID: 27297404.
- A de Rotth, “Plastic repair of conjunctival defects with fetal membranes,” Archives of Ophthalmology, 23, 522 (1940).
- T John, “Amniotic membrane in the surgical management of acute toxic epidermal necrolysis,” Ophthalmology, 109, 351 (2002). PMID: 11825823.
- SCG Tseng, “HC-HA/PTX3 purified from amniotic membrane as novel regenerative matrix: insight into relationship between inflammation and regeneration,” Invest Ophthalmol Vis Sci, 57 (2016). PMID: 27116665.
- K Jirsova, GLA Jones, “Amniotic membrane in ophthalmology: properties, preparation, storage and indications for grafting-a review,” Cell Tissue Bank, 18, 193 (2017). PMID: 28255771.
- T Röck et al., “Amniotic membrane transplantation in reconstructive and regenerative ophthalmology,” Ann Transplant, 23, 160 (2018). PMID: 29507278.
- CT Watson, F Breden, “The immunoglobulin heavy chain locus: genetic variation, missing data, and implications for human disease,” Genes Immun, 13, 363 (2012). PMID: 22551722.
- KN Ma et al., “A novel technique for amniotic membrane transplantation in patients with acute Stevens-Johnson Syndrome,” Ocul Surf, 14, 31 (2016). PMID: 26387869.
- SS Shanbhag et al., “Sutureless amniotic membrane transplantation with cyanoacrylate glue for acute Stevens-Johnson syndrome/toxic epidermal necrolysis,” Ocul Surf, 17, 560 (2019). PMID: 30872140.
- SS Shanbhag et al., “Long-term outcomes of amniotic membrane treatment in acute Stevens-Johnson syndrome/toxic epidermal necrolysis,” Ocul Surf, 18, 571 (2020). PMID: 32200005.
- G Iyer et al., “Treatment modalities and clinical outcomes in ocular sequelae of Stevens-Johnson Syndrome over 25 years – a paradigm shift,” Cornea, 35, 46 (2016). PMID: 26555585.
- TD Papakostas et al., “Prosthetic replacement of the ocular surface ecosystem as treatment for ocular surface disease in patients with a history of Stevens-Johnson syndrome/toxic epidermal necrolysis,” Ophthalmology, 122, 248 (2015). PMID: 25282251.
- SS Shanbhag et al., “A beginner’s guide to mucous membrane grafting for lid margin keratinization: Review of indications, surgical technique and clinical outcomes”, Indian J Ophthalmol, 69, 794 (2021). PMID: 33727438.
- S Basu et al., “Chronic ocular sequelae of Stevens-Johnson Syndrome in children: long-term impact of appropriate therapy on natural history of disease,” Am J Ophthalmol, 189, 17 (2018). PMID: 29421293.
- R Lee et al., “Long-term visual outcomes and complications of Boston Keratoprosthesis Type II Implantation,” Ophthalmology, 124, 27 (2017). PMID: 27538795.
