Cataract surgery has reached a point where every decision - from IOL selection to ocular surface management - directly shapes patient satisfaction and surgical outcomes. As premium cataract procedures become more central to the sustainability of many practices in the era of continued reimbursement cuts, so does the patient experience.
Delivering on a promise
Patients who invest in refractive cataract surgery expect perfect outcomes. Not only do they demand spectacle independence and crisp vision, they want consistency between the vision they were promised and the results they experience. And if there’s one thing that can quietly but profoundly sabotage their result, it’s an unstable ocular surface.
I’ve come to view ocular surface optimization not as a helpful add-on, but as the first critical step in refractive cataract surgery. Obtaining a clear and complete picture of a patient’s ocular surface ensures any issues may be treated aggressively long before surgery. To me, a healthy ocular surface is the difference between meeting a patient’s expectations and explaining away a postoperative refractive surprise. Dry eye disease (DED) causes a greater chance for a 0.50 D or more difference in IOL power (1).
Why ocular surface optimization is no longer optional
Reimbursement for standard cataract surgery continues to decline year after year. Today’s economic reality is pushing practices to convert more patients to premium solutions. Now that more patients choose to pay out of pocket for advanced technology IOLs and laser cataract surgery, there is an even greater responsibility to ensure their biometry is perfect, their surgery is efficient, and their postoperative course runs smoothly.
The challenge is that ocular surface irregularity affects every one of the preoperative measurements that premium outcomes depend mainly on keratometry but also axial length, lens thickness, and anterior chamber depth. These can have a profound impact on IOL selection. When preoperative measurements are not accurate and repeatable, the entire surgical plan is affected.
This is where the comanaging optometrist plays a pivotal role. We are frequently the first provider to catch ocular surface disease (OSD) before it reaches the surgical suite. When optometrists own this step, surgeons get better biometry, patients get better outcomes, and the comanagement relationship is strengthened by a clear and shared standard of care.
Studies show about 80% and 40% of patients presenting for cataract surgery have had at least one or two abnormal tear tests, respectively (2). And even in patients who don’t complain of dry eye symptoms, more than three-quarters (77%) are likely to have corneal staining (3).
Surgeons depend on us to manage the ocular surface before patients arrive for their preoperative consultation. A poorly prepared ocular surface delays their schedule and frustrates everyone involved. Rather than wait for a surgeon’s evaluation to talk to patients about their ocular surface, perform testing ahead of the surgical consultation and prescribe treatment as necessary. By the time a patient sees the surgeon, their ocular surface should be nearly pristine. Aim to obtain two or three stable biometry readings by this time.
Devising a diagnostic and treatment protocol
In southeastern Wisconsin, where the climate is unforgiving and winter seems to last eight months, every patient has dry eye until proven otherwise. Geography aside, OSD is underdiagnosed globally. Optometrists are uniquely positioned to catch it first. Typical complaints include fluctuating vision, burning and stinging eyes, watering, and vague irritation. It also is common for patients to not have any dry eye complaints. It therefore is crucial to look for OSD or lack thereof. When patients come from referring doctors to our practice, however, about 50% arrive with undiagnosed OSD. That’s not a criticism, it’s an opportunity. Optometrists who establish a systematic approach to OSD screening position themselves beyond a referral source. They are indispensable partners in the surgical pathway. Surgeons notice, and they refer back.
I believe a simple diagnostic and treatment protocol is best. A good place to start is by considering the following four steps.
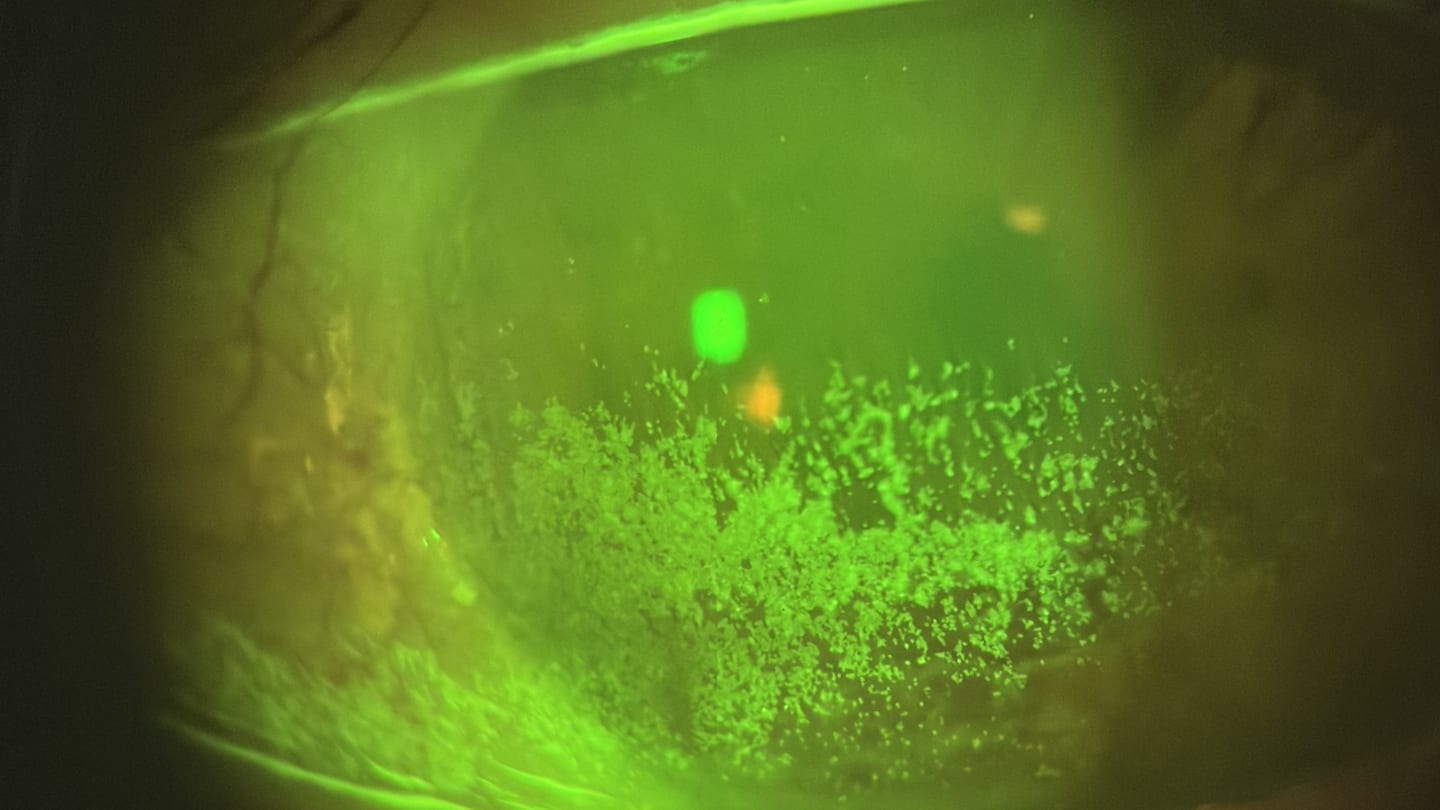
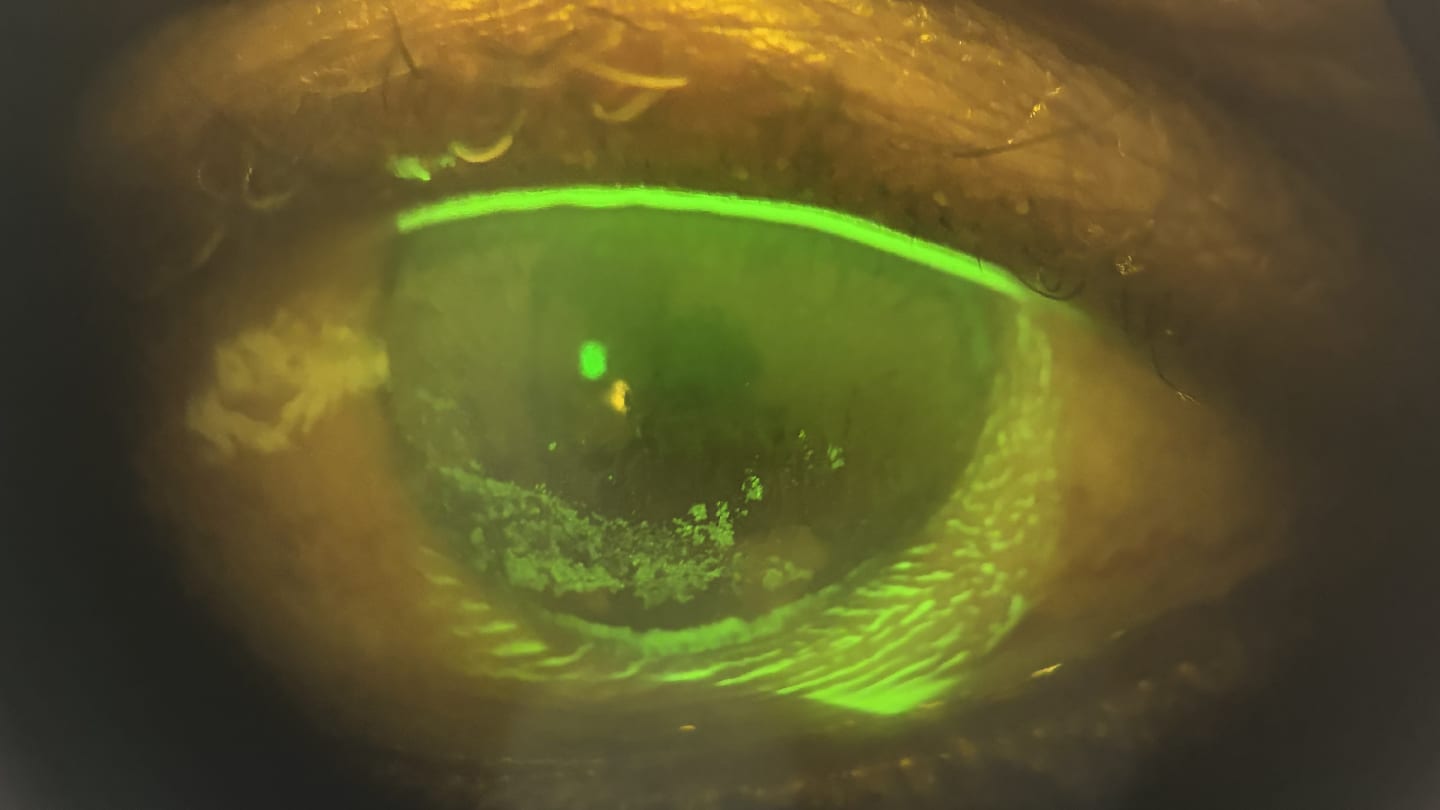
Step 1: Identify symptoms and severity. In most cases, simple tools like OSDI scores, slit-lamp findings, lid margin observations (Figure 1), fluorescein staining (Figure 2), and tear break-up time adequately identify OSD. If aqueous deficiency is suspected, a Schirmer test may be performed.

Step 2: Prioritize treatments that maximize natural tear retention and rapid relief. To improve compliance, it is often helpful to begin with in-office or low-burden treatments that provide durable relief without adding multiple daily drops. Amniotic membranes and lacrimal occlusion are excellent early options. An amniotic membrane can rapidly rehabilitate the ocular surface and reduce inflammation with minimal ongoing effort from the patient, often leading to faster, more noticeable improvement in surface recovery compared to drop therapies that may take weeks to reach full effect. Lacrimal occlusion helps retain the patient’s natural tears, which typically perform better than flooding the eye with artificial tears. This is because the molecular components of natural tears cannot be reproduced commercially. Most patients experience about one week of tearing as the eye equilibrates, followed by meaningful symptomatic improvement. In contrast, topical immunomodulators and other prescription drops, while valuable, often require sustained use and time to work, which can challenge adherence when initiated as the primary therapy.
Step 3: Improve lid margin health. A stable tear film requires healthy lids. Warm compresses with a Bruder mask may be incorporated twice daily. The health of the lid margin may also benefit from hypochlorous acid lid spray and lid wipes for patients with significant debris or Demodex-related complications.
Step 4: Escalate treatment as needed. It is advisable to escalate therapy only when necessary, both to reduce treatment burden and to preserve compliance. Overloading patients with multiple prescriptions may decrease adherence and lead to suboptimal results. If ocular surface inflammation persists despite the above interventions, consider additional treatment in a stepwise fashion. Immunomodulators, anti-evaporative therapies, and other advanced options all have a place in our armamentarium and can be layered according to disease severity and patient response.
The comanagement dividend
When an optometrist takes ownership of ocular surface optimization, the downstream benefits extend well beyond the individual patient. Surgeons who receive patients with repeatable biometry, treated lid disease, and a documented OSD history quickly come to rely on the optometrists who deliver them. That reliance is the foundation of a durable comanagement relationship.
Consider the difference between two referral scenarios.
Scenario 1. A patient arrives at their surgical consultation with an inflamed lid margin, inconsistent keratometry readings, and no prior treatment. The surgeon must now delay the case, initiate treatment, and reschedule. This adds friction to everyone's workflow.
Scenario 2. A patient arrives with two or three stable biometry readings, a completed OSDI, and a documented treatment course. The surgeon can proceed with confidence. In this scenario, the surgeon will remember the optometrist’s preoperative diligence. Additionally, the time investment compounds. Optometrists who consistently deliver optimized patients earn surgical partners who trust their clinical judgment, communicate openly about outcomes, and refer patients back for ongoing care. Ocular surface management isn't just good medicine, it's a practice-building strategy.
Premium lens technology and the ocular surface
Patients electing an advanced technology IOL including toric, multifocal, and adjustable lens designs require careful attention. Ocular surface optimization is even more relevant in these cases. Specifically for the Light Adjustable Lens (LAL; RxSight), an unhealthy cornea and tear film can derail postoperative care.
The latest Light Delivery System enhances efficiency and accuracy of postoperative adjustments, but the entire surgical process still depends on a predictable, stable refraction. As each measurement captures just a moment in time, it is crucial for dry eye to be well-controlled and the cornea optimized.
Treating the ocular surface for about 2 to 3 weeks before preoperative testing improves the opportunity for stable measurements. It also supports optimal healing and minimizes the risk of complications such as infection, scarring, and pain (1). Patients should continue dry eye therapy postoperatively. It should be emphasized to patients that complacency with dry eye drops in this period affects the accuracy of the measurements needed to adjust their IOL appropriately, resulting in adjustment delays, additional visits, and possibly more anxiety.
When patients understand that their ocular surface is the foundation for every adjustment, and when their regimen continues uninterrupted, the LAL journey becomes efficient, accurate, and predictable.
Patient buy-in
Patients who have invested thousands of dollars in premium IOLs or the LAL must embrace the commitment to treating their dryness. I tell them, “You’ve invested in the best possible outcome. You will only achieve that if your ocular surface is healthy. If you skip this step, your outcomes may suffer, not because the technology fails but because the measurements won’t be accurate.”
When framed in terms of protecting their investment and maximizing their results, patients become remarkably compliant. Improving their ocular surface isn’t a cosmetic recommendation, it’s an essential component of the surgical process.
Equally important is communicating to patients that their optometrist and surgeon work together as a coordinated team. When they understand care is continuous, they can feel more confident in the process and more motivated to follow through on treatment.
The new standard of care
Optimizing the ocular surface may not be as glamorous as a femtosecond laser or a novel IOL, but it is the single most important step in giving cataract patients the outcomes they expect. Today, ocular surface optimization shouldn’t just a part of preoperative care, it should be the foundation of refractive cataract surgery. As premium IOLs, light adjustable technology, and laser cataract surgery platforms raise the bar for precision outcomes, optometrists who own the ocular surface become an essential rather than optional member of the care team.
References
- N Venkateswaran et al., "Ocular surface optimization before cataract surgery," Saudi J Ophthalmol., 36, 142 (2022). PMID: 36211316.
- PK Gupta et al., "Prevalence of ocular surface dysfunction in patients presenting for cataract surgery evaluation," J Cataract Refract Surg., 44, 1090 (2018). PMID: 30078540.
- WB Trattler et al., "The Prospective Health Assessment of Cataract Patients’ Ocular Surface (PHACO) study: the effect of dry eye," Clin Ophthalmol., 11:1423 (2017). PMID: 28848324.
