
A visiting surgeon with personal experience of over 100,000 surgical cases recently observed a full day of complex refractive rehabilitation at our practice. The caseload was striking: patients from all over the world with post-PRK haze and scarring, severe post-RK ectasia, failed premium IOLs, contact lens-related corneal infections, and disappointment following Intacs, CAIRS, CTAK, topography-guided laser, and multiple LASIK and SMILE procedures. One patient had been told corneal transplantation was their only remaining option.
After witnessing our LaZrPlastique® approach – an excimer laser procedure that corrects corneal ametropia and abnormalities by refractivity sculpting rather than by cutting the cornea –the visiting surgeon finally asked: “So… LaZrPlastique is not PRK?”
The question stayed with me because it reflects the way refractive surgery has been taught over the last three decades. Surgeons have become extraordinarily sophisticated procedurally and technologically, but possibly limited in the art and science of holistic refractive surgery. Eyes are categorized by procedures, labels, and maps instead of being understood as living and interactive optical systems with visual potential.
Having been involved with LASIK surgery long before its FDA approval in the USA, I have had access to lasers for 30 years (1-3) – even "futuristic" excimer and femtosecond lasers, including those in the beta testing stages. But despite excellent results beyond 20/20 in my LASIK surgical cases, I was becoming a referral center for patients for second opinions and complication management. As I kept seeing these cases, my ongoing drive to custom-design techniques to circumvent their complications made me realize that a cutting procedure would not “cut it.”
I have always felt that cutting into the cornea may weaken it and bring in uncertainties; surely it cannot be applied to a full spectrum of vision corrective populations. Confident in the extraordinary role of our corneal epithelium, and drawing from a wide range of refractive surgical techniques from around the world, I decided that if I had to correct a corneal abnormality, there was no point in cutting and placing back the most important optical layer of the cornea (the anterior cornea). Instead, what if I could sculpt that anterior cornea and then rely on our corneal epithelium to give me the end-healing, circumventing any residual posterior corneal scarring or irregularity? (Not disregarding, of course, the importance of the tear film as an optical element.)
On consenting patients who were referred for corneal transplants by their surgeons, I proceeded to use refraction for these intensely abnormal, scarred, and irregular corneas.
I was fascinated to find that, for each of these patients, this would result not only in good, best-corrected vision, but also excellent unaided vision. This confirmed the concept of not digging after the corneal scars or irregularities, but rather completely disregarding the scars or corneal incisions (like in radial keratotomy, hexagonal keratotomy, or aggressive astigmatic keratotomy). As such, I have never performed a single PTK that was designed to focus on the scar/irregularity rather than on emmetropia.
Many patients had come to me with “successful” topography guided laser surgeries. But where their charts noted success, many did not have unaided vision endpoints. This encouraged me to create algorithms and start treating such patients based on refractive data, while effectively disregarding their topographies, scars, and wave fronts. Instead, I began to carry out surface excimer laser surgery (using the Visx Star S4 laser platform, which has perhaps the longest track record in excimer laser history) with modified algorithms that expanded the application beyond PRK, addressing eyes with abnormal, irregular, and scarred corneas.
That realization became the foundation for LaZrPlastique® (4-5).
LaZrPlastique® was never intended to be used as a marketing term. It is probably one of the least marketable words ever created; it is difficult to pronounce, carries no marketing advantage, and has zero SEO value. Instead, I coined the name to reflect my dedication to raising eye surgery beyond machine-based numbers and limitations – and into pure surgical artistry aimed towards unaided emmetropia and vision.
This is not to reject PRK (6), PTK, EpiLasik, and other surface laser surgeries as we know them; it is an attempt to custom-design and expand upon them. In fact, LaZrPlastique® has been used to correct side effects and complications of PRK itself. Additionally, it has been successfully used to correct Herpes corneal scars (off label), which is a contraindication for PRK.
Over time, I have applied this approach to patients arriving not only for refractive correction, but for refractive rescue (7-9) – patients with starbursts, glare, flap complications, irregular astigmatism, ghosting, decentered ablations, progressive ectasia, fluctuating vision, and failed enhancements. Many had already undergone multiple procedures elsewhere and had been advised to “learn to live with it" (10).
But, once one stopped looking just at anatomy, many of these eyes still possessed remarkable refractive potential. The cornea, from this perspective, is not merely tissue; it is optical architecture.
Every cornea carries biomechanical memory, epithelial compensation, healing behavior, asymmetry, lenticular interaction, and a refractive personality unique to that eye. Topography may describe shape, but refraction still describes human vision. A topography may appear smooth while the patient remains visually disabled, but another eye may appear anatomically chaotic while still maintaining refractive logic capable of rehabilitation. This observation became one of the core principles behind LaZrPlastique®.
Historically, corneal scars have pushed surgeons toward structural thinking: remove the opacity, smooth the surface, and transplant the tissue. Yet over decades of tertiary referrals from around the world, I have repeatedly encountered scarred corneas that still refracted remarkably well despite their dramatic appearance.
This led to a refractive approach to corneal scars - "In-Cornea Scars" – in which selected scars are viewed not simply as structural abnormalities but as part of the cornea's optical system.
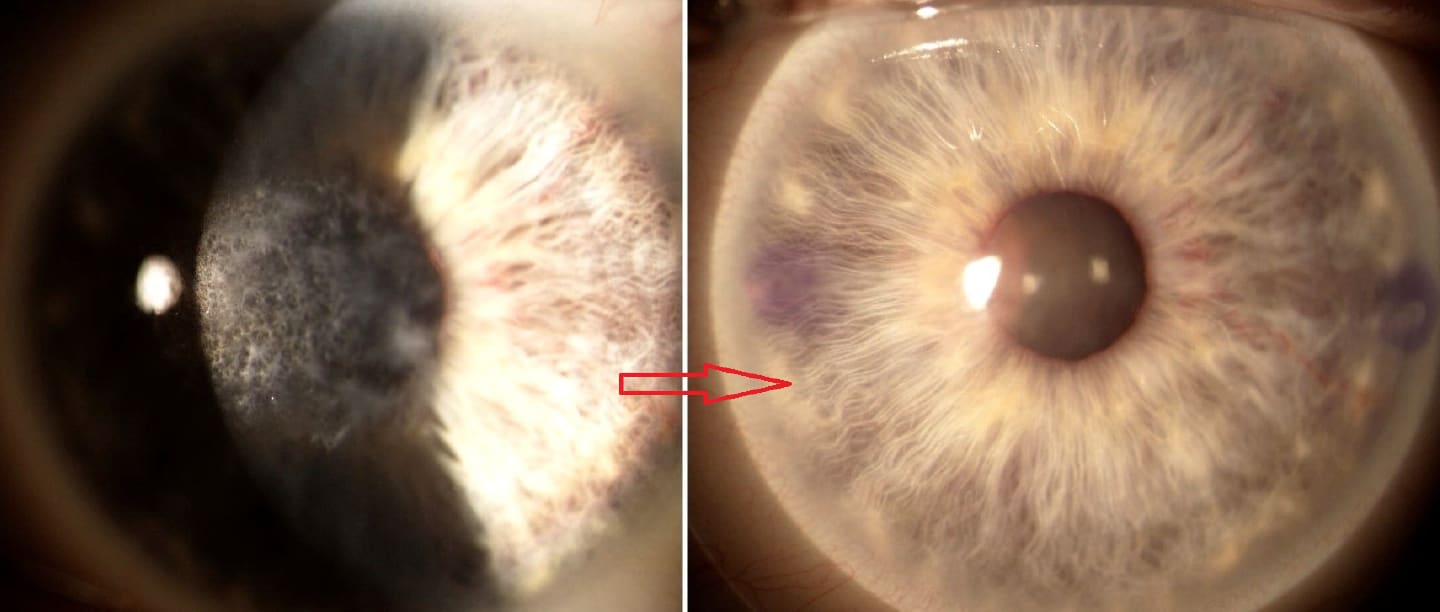
In a 21-year series of 73 eyes with corneal scars from 27 different etiologies, including infectious, traumatic, post-refractive surgery, and ectatic conditions, visual rehabilitation was pursued from a refractive rather than purely anatomical perspective. Using conservative excimer laser corneoplastique techniques, 93% of eyes achieved 20/30 or better uncorrected vision, with no reported cases of haze, infection, ectasia, or scar recurrence. These findings support the concept that carefully selected corneal scars can often be managed as refractive problems rather than solely as anatomical defects (11).
What interested me most was not simply the visual outcome, but the implication. Many scarred corneas are not purely opacity problems – they are refractive problems hidden within opacity.

Impact on global eye health
That distinction may have enormous implications globally. Corneal scarring remains one of the leading causes of avoidable blindness worldwide (12), and yet donor tissue availability, transplant infrastructure, long-term postoperative management, and immunologic challenges remain major limitations. If selected scarred corneas can instead undergo refractive optical rehabilitation while preserving native tissue, the future of corneal blindness management may not rely exclusively upon replacement surgery. Perhaps, in selected eyes, the answer lies in rehabilitating the optics already present.
Democratizing laser refractive surgery
However, the larger purpose of LaZrPlastique® extends beyond scars, LASIK, or even refractive surgery itself. It is educational.
For decades ophthalmology has divided itself into procedural silos — cornea surgeons, cataract surgeons, refractive surgeons, ocular surface specialists, transplant surgeons. But patients, do not experience vision in silos. They arrive with one visual system and one desire: to function normally again.
I believe the future eye surgeon must evolve into a “full-spectrum vision corrective surgeon" - someone capable of understanding cornea, lens, optics, ocular surface disease, irregular astigmatism, refractive architecture, healing behavior, and visual quality, including staged manipulations of optics, as one interconnected system. Not a surgeon who performs one procedure repeatedly, but one who designs vision for each case uniquely.
This is particularly important today because modern patients are no longer presented with isolated pathology. We increasingly see layered optical situations and complexities (e.g.for post-LASIK irregular astigmatism with corneal ectasia, unhappy premium lens cataract surgery cases, RK instability with irregular astigmatism, keratoconus combined with lenticular dysfunction, and post-SMILE aberrations combined with ocular surface instability). These eyes demand refractive thinking that transcends procedural categories.
In fact most of the "20/Unhappy" premium lens cataract surgery patients that are referred to me have not had to go back under the knife for their surgeon’s lens exchange. Instead, I have corrected their lens implant issues by manipulating the optics with LaZrPlastique® on their cornea and restoring their optical coherence to "20/20/Happy" (13).
This is why LaZrPlastique® is not just a procedure to me. It is an expanded application spectrum of surface laser surgery, a refractive mindset that reflects my desire to raise refractive surgery to an art, and encourage and empower every eye surgeon to become a full-spectrum vision corrective surgeon.
References
- AC Gulani, “New Triple Benefit Intra-Ablative Contact Lenses for Hyperopic LASIK,” Contactologica, 21, 107 (1999).
- AC Gulani, “Corneoplastique,” Video Journal of Cataract and Refractive Surgery, 22(3) (2006).
- AC Gulani et al., “Wavefront in LASIK: The Zyoptix Platform,” Ophthalmol Clin N Am, 17, 173 (2004). PMID: 15158963
- AC Gulani et al., “LaZrPlastique®: Pioneering a New Era in Laser Vision Surgery for Universal Application and Democratization of Refractive Surgery,” Indian J Cataract Refract Surg (2025).
- AC Gulani, “LaZrPlastique®: The Non-Cutting Edge Over LASIK,” Ophthalmology Times (2025).
- CR Munnerlyn et al., “Photorefractive Keratectomy: A Technique for Laser Refractive Surgery,” J Cataract Refract Surg, 14, 46 (1988). PMID: 3339545
- A Gulani, “Principles of Surgical Treatment of Irregular Astigmatism in Unstable Corneas,” in Textbook of Irregular Astigmatism Diagnosis and Treatment, SLACK Incorporated, 251–261 (2007).
- AC Gulani, “Corneoplastique®: Art of Vision Surgery,” Indian J Ophthalmol, 62, 3 (2014). PMID: 24492591
- A Gulani, “Corneoplastique®,” Tech Ophthalmol, 5, 11 (2007).
- A Gulani, “A Refractive Approach for Irregular and Scarred Corneas to 20/20 Unaided Vision: LaZrPlastique,” presented at ASCRS Annual Meeting, Washington, DC (2026).
- AC Gulani et al., “Corneoplastique™ for Corneal Scars: Treating Corneal Scars as Refractive Errors – A 21-Year Experience,” Clin Ophthalmol, 18, 2927 (2024). PMID: 39418057
- JP Whitcher et al., “Corneal Blindness: A Global Perspective,” Bull World Health Organ, 79, 214 (2001). PMID: 11285665
- AC Gulani, “Premium Lens Cataract Surgery: Addressing Unhappy and ‘Complications’ Patients for Eye Surgeons: An Innovative Approach to Restoring Vision Without Going Back Under the Knife,” The Ophthalmologist (January 2025).
