
Dear cataract surgeon colleagues,
Advances in intraocular lens (IOL) and surgical technologies have made modern cataract surgery a transformative procedure that can safely and predictably restore vision within a matter of minutes. With innovations like artificial intelligence-designed optics(1) and femtosecond laser-assisted surgery (2), cataract surgeons today can achieve near-perfect postoperative vision, something which can be less frequent in complex retinal surgery.
Of course, this assumes the eye is otherwise healthy without underlying conditions that might compromise vision. While patients with established retinal disease are usually under the care of a retina specialist by the time they present for cataract surgery, other seemingly healthy patients could be harboring subtle, early-stage retinal lesions that are clinically silent or challenging to visualize through media opacity. Undiagnosed or untreated retinal pathology can jeopardize postoperative outcomes and patient satisfaction, undermining even a technically flawless cataract surgery. Therefore, cataract surgeons must maintain a high index of suspicion and include a thorough retinal evaluation in their preoperative workflow for optimum outcomes following cataract surgery.
Pre-operative screening
The gold standard in retinal examination comprises slit-lamp examination of the posterior pole and evaluation of the retinal periphery with indirect ophthalmoscopy (IDO) and scleral depression. However, the latter method can be technically challenging nowadays, especially for the younger generation that is less exposed to it. Moreover, peripheral retinal lesions are easy to overlook, especially when obscured by lens opacities or inadequate pupillary dilation. This can have vision-threatening consequences; for example, untreated peripheral retinal tears can precipitate retinal detachments (RD) post-cataract surgery (3). Cataract surgery itself can precipitate posterior vitreous detachment (PVD)leading to retinal breaks and RD (4, 5), which further emphasizes the importance of a complete, panretinal pre-operative examination. Traditional examination methods are also time-consuming and require high-level expertise, meaning the process often rests solely on the ophthalmologist with little opportunity for delegation, making them less practical for routine screening in high-volume clinics.
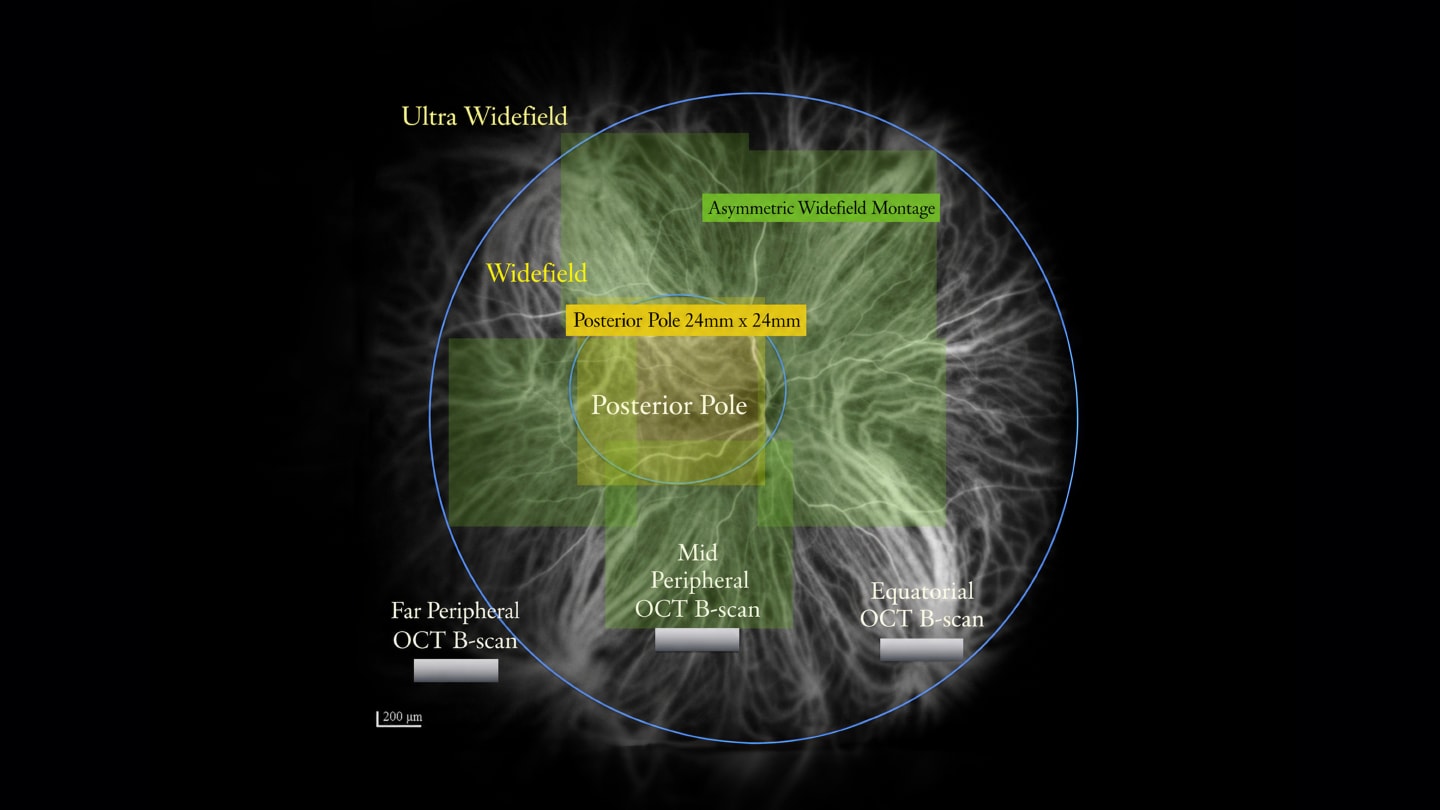
For efficient yet extensive retinal evaluation, digital retinal imaging can be a useful alternative. Whilst color fundus photography (CFP) and optical coherence tomography (OCT) have long been the standard in posterior pole assessment, growing evidence on the clinical significance of peripheral retinal changes has driven increased adoption of widefield (WF) and ultra-widefield (UWF) imaging with wider fields of view (FOVs) than the 30°–75° FOV afforded by CFP (6, 7). WF imaging captures the retina posterior to the vortex vein ampulla, while UWF imaging provides a panoramic view of the retina beyond the vortex vein ampulla till the pars plana (Figure 1) (8). Commercially available WF imaging devices include the iCare EIDON with a 90° single-image FOV (iCare Finland Oy, Vantaa, Finland) and the Clarus 700 with a 133° single-image FOV (Carl Zeiss, Dublin, CA). For UWF imaging in our clinic, we use the Optos California (Optos, Dunfermline, UK) that captures 200° optomap images of the retina in a single image (not montaged), making it the largest FOV in the market (9). Optomap devices utilize confocal scanning laser ophthalmoscopy to penetrate media opacities like dense cataracts, enabling retinal visualization in 85% of cases (10). Combined with the broad FOV, these devices support the detection of peripheral retinal lesions that might otherwise go unnoticed.
In busy practices, WF and UWF devices enable efficient delegation, as trained staff can acquire preliminary retinal scans which are then reviewed by ophthalmologists for image-guided retinal assessments. This optimized workflow not only increases diagnostic accuracy but also converts consultations into opportunities for patient education. Using the acquired images, surgeons can visually explain retinal findings to patients, supporting better expectation-setting and informed decision-making ahead of cataract surgery.
There is a vast range of retinal conditions that can be difficult for the non-retina specialist to diagnose before cataract surgery. Lesions such as subclinical macular edema (ME), vitreomacular traction, and lamellar macular holes can be unapparent to the non-retina specialist on CFP, especially when obscured by lens opacity. Additional tests like OCT may be needed to confirm the respective contributions of the cataract and the macula to patients’ visual complaints. OCT is often employed with CFP in conditions predisposing to MO, like diabetic retinopathy (DR) and age-related macular degeneration (AMD). In vascular disorders such as retinal vein occlusions (RVO) and DR, fundus fluorescein angiography (FFA) can also be helpful in identifying the extent of retinal ischemia. Some WF and UWF imaging systems offer an advantage by allowing multimodal retinal evaluation with a single device, like the Clarus 700 with WF color, autofluorescence, and FFA imaging modalities, and the Silverstone RGB with single-capture UWF color, autofluorescence, FFA, and navigated swept-source OCT (posterior pole and peripheral) imaging capabilities (11, 12).
In eyes with advanced cataracts completely obscuring the fundus view, some surgeons may still opt to conduct B-scan ultrasonography to rule out gross pathology such as vitreous hemorrhage or retinal detachments that can affect treatment planning and outcomes.
Surgical planning and legal considerations
Fundus imaging - including WF and UWF imaging - facilitates documentation of examination findings for medicolegal purposes. High-quality, timestamped digital images provide an objective record of preexisting pathology, helping clarify the baseline status should outcomes fall short of expectations. This can be critical in addressing patient concerns, defending clinical decisions, and reducing liability. Based on the retinal findings, cataract surgeons can also tailor surgical plans and collaborate with retina specialists as needed.
A coexisting retinal pathology may change the surgical planning and visual prognosis, and some lesions will need to be addressed by the retina specialist prior to cataract surgery. The release of inflammatory and angiogenic factors following cataract surgery can aggravate diseases such as diabetic macular edema (13). Some conditions may require to be treated with anti-VEGF (vascular endothelial growth factor) agents until the lesions are stable, before embarking on cataract surgery. There are no concrete guidelines for the timing of cataract surgery after retinal stabilization, so the decision to operate may be made after due consultation with the retina specialist. Peripheral high-risk lesions predisposing to RD should be pre-operatively treated with laser photocoagulation, and cataract surgery should be planned after adequate pigmentation of the treated area has developed (3).
The right IOL with the appropriate surgical procedure and follow-up
Concomitant retinal examination can also guide IOL selection. Premium presbyopia-correcting IOLs like diffractive multifocal IOLs can reduce contrast sensitivity, compounding the visual quality impairments in macular diseases like AMD and epiretinal membrane (ERM) (14). Lesions such as macular holes or ERM may require vitrectomy in the future, so it is best to avoid silicone or hydrophilic acrylic IOLs in these cases as they may develop IOL opacifications following intravitreal silicone oil or gas tamponade (15).
The cataract surgery procedure itself may need to be modified in certain conditions. Patients with ERM or DR have a higher risk of developing ME post-operatively, so surgeons should reduce surgical trauma and inflammation through the use of low flow and turbulence parameters, and reduced phaco energy. Similar phaco system parameters should also be used in patients with retinal ischemia. Patients with ERM may even benefit from a combined approach of cataract surgery and vitrectomy with ERM peel, ideally performed by a vitreoretinal surgeon also competent in cataract surgery. Perioperative topical NSAIDS (nonsteroidal anti-inflammatory drugs) and steroids can be administered to further reduce the risk of ME (16). Unnecessary light exposure should be avoided in AMD to prevent phototoxic injury.
Following cataract surgery, close follow-up with serial dilated fundoscopy allows early detection of complications. Non-mydriatic WF or UWF imaging shows good consistency with dilated examination(17, 18) and can be utilized for quick and convenient follow-ups. Additionally, serial OCT scans can aid in monitoring macular thickness and titrating topical anti-inflammatory therapy. UWF technologies with navigable OCT imaging like the Silverstone RGB can visualize the vitreoretinal interface from the posterior pole to the far periphery (Figure 2),(12), enabling early detection of PVD and retinal breaks secondary to the vitreous destabilization associated with cataract surgery.
In summary, retinal examination should be an integral part of the cataract surgery equation. Tools like UWF imaging can be useful adjuncts to clinical examination and are poised to further optimize patient flow and clinical diagnoses. By leveraging these systems, cataract surgeons can incorporate detailed retinal evaluations into routine workflows and collaborate efficiently with retina specialists. As cataract surgeons continue to push the boundaries in the pursuit of the best possible outcomes, they may find that the answer to optimizing vision could, sometimes, lie beyond the lens.

Images courtesy of Paulo-Eduardo Stanga, MD.]
References
- S Mantry et al., “IOL Design Puts a New Spin on Vision,” Ophthalmology Times Europe (February 2025). Accessed April 9, 2025.
- X Chen et al., “Cataract: Advances in Surgery and Whether Surgery Remains the Only Treatment in Future,” Adv Ophthalmol Pract Res, 1, 100008 (2021). PMID: 37846393
- R Venkatesh et al., “Recommendations for Management of Peripheral Retinal Degenerations,” Indian J Ophthalmol, 70, 3681 (2022). PMID: 36124501
- S Hayashi et al., “Progression of Posterior Vitreous Detachment After Cataract Surgery,” Eye, 36, 1872 (2022). PMID: 34413336
- JH Park et al., “Risk Factors for Onset or Progression of Posterior Vitreous Detachment at the Vitreomacular Interface After Cataract Surgery,” Ophthalmol Retina, 5, 270 (2021). PMID: 32800897
- V Kumar et al., “Ultra-Wide Field Retinal Imaging: A Wider Clinical Perspective,” Indian J Ophthalmol, 69, 824 (2021). PMID: 33727498
- PE Stanga, “Update on Imaging the Peripheral Retina,” Saudi J Ophthalmol, 38, 99 (2024). PMID: 38988789
- N Choudhry et al., “Classification and Guidelines for Widefield Imaging,” Ophthalmol Retina, 3, 843 (2019). PMID: 31474489
- PE Stanga et al., “New 200° Single-Capture Color Red-Green-Blue Ultra-Widefield Retinal Imaging Technology: First Clinical Experience,” Ophthalmic Surg Lasers Imaging Retina, 54, 714 (2023). PMID: 37991593
- WS Chen et al., “Advances in Retinal Imaging of Eyes with Hazy Media: Further Studies,” Invest Ophthalmol Vis Sci, 52, 4036 (2011).
- A Saladino et al., “Value of Combining Ultra-Widefield Fundus Fluorescein Angiography (UWF-FFA) with 130° Single-Scan Ultra-Widefield Optical Coherence Tomography Angiography (UWF-OCTA) in Retinal Vasculopathies,” Retina (2026). PMID: 41666370
- PE Stanga et al., “The Role of Ultra-Widefield Imaging with Navigated Central and Peripheral Cross-Sectional and Three-Dimensional Swept Source Optical Coherence Tomography in Ophthalmology: Clinical Applications,” Saudi J Ophthalmol, 38, 101 (2024). PMID: 38988788
- TY Wong et al., “Guidelines on Diabetic Eye Care,” Ophthalmology, 125, 1608 (2018). PMID: 30097331
- E Yeu, S Cuozzo, “Matching the Patient to the Intraocular Lens: Preoperative Considerations to Optimize Surgical Outcomes,” Ophthalmology, 128, e132 (2021). PMID: 32980322
- A Grzybowski et al., “A Narrative Review of Intraocular Lens Opacifications: Update 2020,” Ann Transl Med, 8, 1547 (2020). PMID: 33313100
- BA Henderson et al., “Clinical Pseudophakic Cystoid Macular Edema,” J Cataract Refract Surg, 33, 1550 (2007). PMID: 17720069
- B Abadia et al., “Non-Mydriatic Ultra-Wide Field Imaging Versus Dilated Fundus Exam and Intraoperative Findings for Assessment of Rhegmatogenous Retinal Detachment,” Brain Sci, 10, 521 (2020). PMID: 32756550
- SKH Szeto et al., “Non-Mydriatic Ultrawide Field Scanning Laser Ophthalmoscopy Compared with Dilated Fundal Examination for Assessment of Diabetic Retinopathy and Diabetic Macular Oedema in Chinese Individuals with Diabetes Mellitus,” Br J Ophthalmol, 103, 1327 (2019). PMID: 30487128
