- Small pupils can present a big challenge – particularly in femtosecond laser-assisted cataract surgery (FLACS)
- Inadequate pupil dilation during cataract surgery may lead to serious intraoperative complications
- Pupil expansion devices are an excellent method of increasing and maintaining pupil size during FLACS
- Tips and tricks for the best-possible usage of the Malyugin Ring before and during FLACS are explored
Performing cataract surgery in patients with a small pupil size is undoubtedly a challenge. Inadequate pupil dilation during cataract surgery – which usually occurs in patients with conditions such as glaucoma, pseudoexfoliative syndrome, chronic uveitis, and diabetes mellitus – may lead to serious intraoperative complications, including iris damage, bleeding and prolapse, intraoperative floppy iris syndrome (IFIS), anterior capsule damage and potential misalignment of the intraocular lens (IOL). Fortunately, cataract surgeons have access to a number of surgical techniques and devices that can minimize the risk of complications by aiding pupil dilation: viscomydriasis, iris retractor hooks and intracameral injection of adrenergic receptor agonists, to name but a few.
The challenge of small pupil size
It has been said that femtosecond laser-assisted cataract surgery (FLACS) has the potential to revolutionize cataract surgery. Although there’s a growing body of evidence to suggest that, compared with manual phacoemulsification, FLACS increases safety, accuracy, and improves clinical outcomes, it’s certainly not immune to complications (1,2). The problems associated with performing phacoemulsification in patients with small pupils remain, and may even be amplified, particularly during the early learning curve. The application of laser energy can lead to pupillary miosis – in some cases constricting pupil size down to 3.0 mm between applanation with the patient interface and initiation of phaco. This is more pronounced if the surgeon opts for a non-optimal preoperative medication protocol and when the laser is shooting very close to the pupillary margin. In some cases, miosis induced during FLACS may lead to damage of the pupillary border during lens aspiration. Consequently, FLACS is contraindicated in patients with pupils smaller than 5.0 mm in diameter (1). However, even if a patient meets the inclusion criteria for FLACS, surgeons should have access to a reliable and efficient method of ensuring and maintaining adequate pupil dilation so that patients can reap the benefits, rather than the complications, associated with the procedure.Employing the Malyugin Ring
In my practice, I take a step-by-step approach to increase and maintain pupil size during FLACS. First, preoperative mydriatics should be combined with instillations of nonsteroidal anti-inflammatory drugs to prevent the pupil from constricting between the laser and the surgical steps of the FLACS procedure. If, after the laser step, the patient’s pupil is not optimal in size, I start with intracameral mydriatics such as non-preserved, bisulfate-free phenylephrine 1.5%, eventually leading up to the use of a pupil expansion device if necessary. There are a number of pupil expansion devices on the market, including the Graether Pupil Expander (Eagle Vision Inc.), the Type 5S Iris Ring (Morcher GmbH), the Oasis Iris Expander and the Xpand Iris Expansion System (Diamatrix). My preference, obviously, is the Malyugin Ring (MicroSurgical Technology), a pupillary expansion device that I developed in order to avoid the disadvantages associated with some pupil expanders – such as potential overstretching of the iris sphincter or extended surgery time. The Malyugin Ring, which is available in diameters of 6.25 and 7.0 mm, is a square-shaped implant with four paper clip-like circular scrolls that provide eight points of fixation (Figure 1). This unique design ensures uniform dilatation of the pupil and circumferential protection of the iris. A key advantage of the Malyugin Ring is that it can be placed through the main incision (2.2 mm), thus eliminating the need to create extra incisions like those necessary with the use of iris hooks. Importantly, it is less likely to damage the iris sphincter than other corneal rings, as it affords only minimal contact with the iris. Additionally, because it has a thinner profile (<1.0 mm) than other pupil expansion rings, it is less likely to cause the iris to “tent,” which in turn reduces the chance of viscoelastic becoming trapped underneath.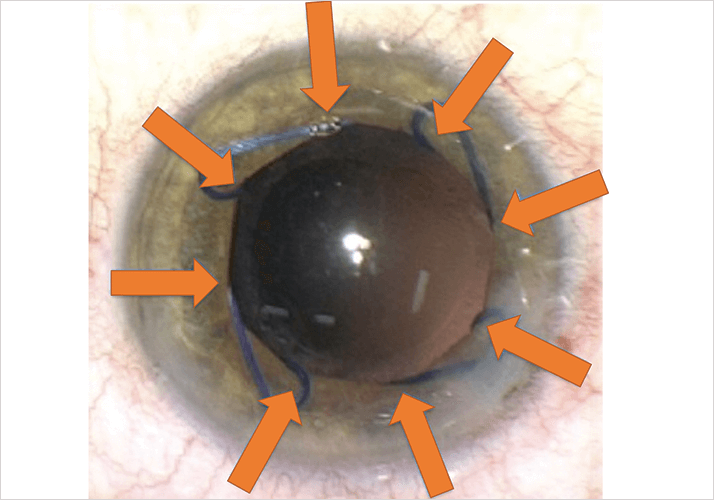
The Malyugin Ring is supplied with its own injector, used to both place and remove the ring, which saves considerable time during placement and removal relative to other pupil expansion devices. The injector needs a corneal incision that is at least 2.2 mm wide but, utilizing a wound-assisted injection technique where the corneal tunnel is used as an extension of the injector tube, it is possible to implant the ring through an incision as small as 1.8 mm. Because the Malyugin Ring is available in two sizes, it offers the cataract surgeon more flexibility. For instance, although the 6.25 mm ring can be used in most cases (it’s easier to implant and remove than the 7.0 mm ring), the larger ring can be effectively employed in IFIS, and is also more compatible with certain phacoemulsification techniques such as the divide-and-conquer and phaco-flip. There is also growing evidence that the Malyugin Ring is a reliable and stable method of maintaining an adequate surgical pupil diameter during FLACS (4), allowing patients who might not normally be considered for FLACS to benefit from this procedure.
Tips and techniques
When implanting the Malyugin Ring after the anterior capsulorhexis has been performed, there is the possibility that you might catch the capsular edge with one or more of the scrolls. To avoid that issue, I prefer to use highly viscous ophthalmic viscosurgical device (OVD, Healon 5 [2.3%, sodium hyaluronate, AMO]) and inject it behind the iris in four points corresponding to the future position of the scrolls on the iris margin. In my experience, the regular cohesive OVD (1% sodium hyaluronate) usually does not provide sustainable iris lifting. When injecting the leading scroll, I like to position the injector tip very close to the iris margin. This helps to better control engagement of the scroll with the iris. Then, while the ring is injected, the injector is slowly retracted back in the direction of the main incision. The two side scrolls (usually simultaneously) catch the iris, and the last scroll is disengaged from the injector hook and positioned in place with the help of the ring manipulator (Lester or Kuglen hooks).The next step is critical, as I want to be sure that the ring is not engaging the anterior capsulorhexis margin. For this, a “picture frame” maneuver is very useful. By using the sideport instrument, it is quite easy to displace the ring in any direction, very much like a picture frame. The direction in which movement is restricted usually corresponds to the scroll that is catching the anterior capsule. After you recognize this, it’s quite easy to go in with the ring manipulator, catch the scroll, retract it towards the center of the anterior chamber, disengage from the iris (and capsule), and then lift it a little bit and position it back in contact with the pupillary edge. This technique can obviously be repeated if more than one ring scroll is catching the anterior capsule. And then, finally, the “picture frame” maneuver is repeated to ensure the correct position of the Malyugin Ring.
Luckily in FLACS the anterior capsulorhexis rim has a specific greyish-white color and can be much better visualized than with manual capsulorhexis, thus further minimizing the risk of this complication as compared with conventional phaco. It’s crucial that the OVD is removed from the anterior chamber completely after Malyugin Ring implantation, otherwise residual particles of viscoelastic attached to the anterior lens capsule may lead to incomplete capsulotomy and create capsular “bridges” (3).
Clinical evidence and surgical technique
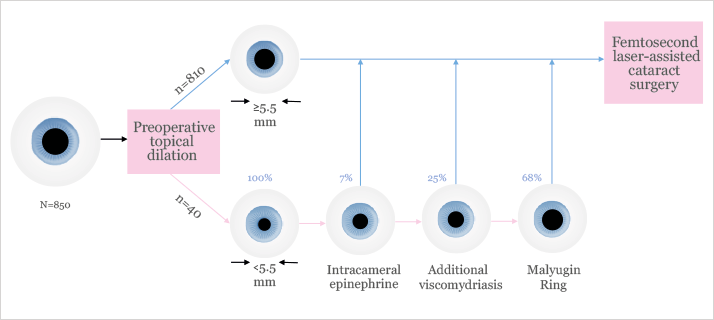
In a case report published in the Journal of Clinical and Experimental Ophthalmology in 2013 (4), Jirasková et al. described a technique that allows surgeons to perform FLACS with the LenSx laser (Alcon) in patients with poor- or non-dilating small pupils, reporting “excellent” results. In this case, the Malyugin Ring was implanted (using the injector supplied with the ring) into the anterior chamber after creation of a 2.2 mm incision and filling the anterior chamber with a cohesive OVD (Provisc [1.0% sodium hyaluronate], Alcon). A 4.8 mm diameter circular capsulotomy was then performed, followed by nucleus fragmentation; then, after implanting the IOL into the capsular bag, the Malyugin Ring was easily removed using the injector under OVD to protect the corneal endothelium. The authors note that by using the Malyugin Ring, a uniform and gentle dilation of the pupil was achieved and that this particular ring proved to be a “reliable and stable” method of maintaining an adequate surgical pupil diameter during each stage of FLACS.Ina Conrad-Hengerer and her colleagues have also described the use of the Malyugin Ring during FLACS (5). In an 850-eye prospective clinical trial undertaken at Ruhr University Eye Clinic, Bochum, Germany, patients with a pupil size smaller than 5.5 mm received sequential treatments to increase pupil size to over 5.5 mm, i.e., administration of epinephrine solution, additional viscomydriasis, and implantation of a Malyugin Ring. The authors reported that epinephrine was sufficient in only 7 percent of eyes, while additional viscomydriasis was necessary in 25 percent and the pupil expander was implanted in 68 percent of cases (Figure 2). Consequently, this three-step pupil dilation procedure culminating in use of the Malyugin Ring allowed the surgeon to increase the efficacy and safety of FLACS in eyes with a small preoperative pupil. Dick et al. also used the Malyugin Ring in a 73-eye study of FLACS in patients with small pupils. The authors reported that laser treatment was viable in all cases after mechanical dilation of the pupil, either using iris retractors or a Malyugin Ring. Moreover, there were no instances of flattening of the anterior chamber or any other complications (6).
These early findings suggest that the Malyugin Ring could play an important role in FLACS by helping to overcome the challenges associated with performing the procedure in patients who have small or poorly dilating pupils. Importantly, the Malyugin Ring may also provide patients previously deemed unsuitable for FLACS with the opportunity to reap the safety and efficacy benefits of this technology.
Boris Malyugin is a professor of ophthalmology and the Deputy Director General at the S. Fyodorov Eye Microsurgery State Institution, Moscow, Russia.
References
- KE Donaldson, et al., “Femtosecond laser-assisted cataract surgery”, J Cataract Refract Surg, 39, 1753–1763 (2013). PMID: 24160384. KM Hatch, JH Talamo, “Laser-assisted cataract surgery: Barriers of the femtosecond laser”, Curr Opin Ophthalmol, 25, 54–61 (2014). PMID: 24248094. DS Grewal, S Basti, “Incomplete capsulotomy using femtosecond laser with a pupil expansion device”, J Cataract Refract Surg, 40, 680–682 (2014). PMID: 24680522. N Jirasková, et al., “Use of Malyugin pupil expansion ring in femtosecond laser-assisted cataract surgery”, J Clin Exp Ophthalmol, 4, 312 (2013). I Conrad-Hengerer, et al., “Femtosecond laser-assisted cataract surgery in eyes with a small pupil”, J Cataract Refract Surg, 9, 1314–1320 2013). PMID: 23988243. HB Dick, T Schultz, “Laser-assisted cataract surgery in small pupils using mechanical dilation devices”, J Refract Surg, 29, 858–862 (2013). PMID: 24404609.
