Nearly 10 million cataract surgeries are performed worldwide each year (1), with costs to both providers and patients varying widely based on location. One expenditure that could be eradicated is that of routine preoperative testing (including, but not limited to, blood counts, chemical analyses, coagulation studies, urinalysis, electro- or echocardiography, cardiac stress tests, chest radiography and pulmonary function tests). Such testing is not recommended for patients undergoing cataract surgery because it neither improves outcomes nor reduces the incidence of adverse events. In a recent paper in the New England Journal of Medicine, a group from the University of California, San Francisco investigated how well medical practices adhere to this recommendation, how much unnecessary testing is costing the healthcare system, and what characteristics might be associated with unnecessary testing.
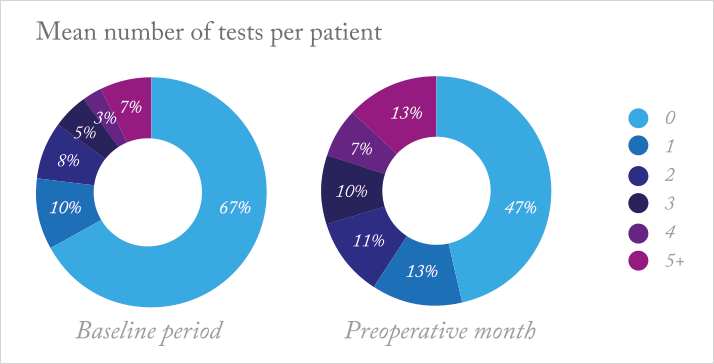
The researchers observed a cohort of Medicare beneficiaries undergoing cataract surgery to determine the prevalence and cost of testing administered in the month leading up to surgery (as compared to the 11 months before). After gathering data, they used statistical analyses to examine the relationship between preoperative testing and a variety of patient and provider characteristics. Over half of the 440,857 patients had at least one test in the month before surgery (2), with a significant proportion having multiple tests (see Figure 1). A patient’s probability of being tested was found to be associated mainly with the ophthalmology practice managing their preoperative care – 36 percent of ophthalmologists ordered tests for more than 75 percent of their patients, and 8 percent had all of their patients tested. There were significant increases in cost, too; expenditures on testing rose by US$4.8 million in that month as compared with the preceding 11 months, and expenditures on office visits by US$12.4 million.
It’s clear that preoperative testing is still common among US ophthalmology practices, though the factors driving testing despite recommendations against it are less obvious. But given the high price of these unnecessary tests, a useful next step would be to determine why they’re still being prescribed, and what can be done to more effectively discourage their use.
References
- A Foster, “Vision 2020: the cataract challenge”, Community Eye Health, 13, 17–19 (2000). PMID: 17491949. CL Chen, et al., “Preoperative medical testing in Medicare patients undergoing cataract surgery”, N Engl J Med, 372, 1530–1538 (2015). PMID: 25875258.
