Cataract surgery is one of the most performed surgeries in the world, so it is vital to ensure it is a success for both the surgeon and patient. Using lower intraocular pressure (IOP) during surgery is important as it may help preserve eye health. The challenge is to achieve this while increasing surgical efficiencies and improving anterior chamber stability.
Achieving lower IOP, working with Centurion® Vision System (1) with ACTIVE SENTRY® Handpiece, brings multiple benefits, including increasing surgical efficiency and anterior chamber stability and reducing the risk of ocular blood flow (2) and corneal endothelium damage, that can occur with high IOP (3, 4). Both of these serious adverse consequences have a real potential to come back to haunt surgeons, as it may result in unsuccessful surgery with poor patient outcomes, if not proactively addressed by working at lower IOP.
“We are finding working at lower IOP with the ACTIVE SENTRY® Handpiece helps surgeons operate with far greater confidence,” says Professor Daniele Tognetto, Chairman of the University Eye Clinic of Trieste, Italy. “These technologic advancements can promise patients more positive outcomes with lower rates of complications.”
Launched in 2019 as part of the Centurion® Vision System, the ACTIVE SENTRY® Handpiece (working together with ACTIVE FLUIDICSTM) has been designed by Alcon to enable surgeons to control intraocular IOP during surgery. The ACTIVE SENTRY® Handpiece contains an integrated pressure sensor detecting fluctuations in real-time. Previously, pressure alterations at the tip of the phaco probe travelled to a sensor located inside the cassette at the speed of sound. Having the sensor located inside the handpiece eliminates millisecond delays in adjusting fluidics and avoids dramatic drops in IOP.
Alcon’s ACTIVE FLUIDICSTM technology replaced traditional gravity-based phaco fluidics. The system compresses a bag of balanced salt solution to overcome infusion line resistance as aspiration flow varies.
In the gravity system there is the delay given by the length of the tube (at least 1.20 m from the balanced salt solution to the Fluidic Management system + 1.20 m from the Fluidic Management system to the patient’s eye). With ACTIVE SENTRY® there is no delay since the sensor is inside the Handpiece.
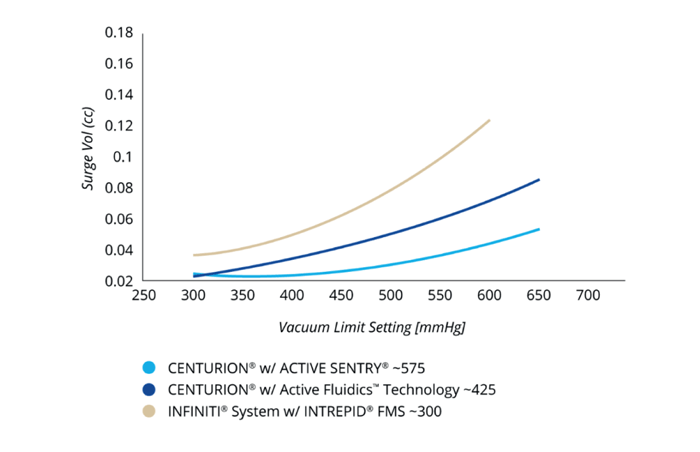
Working together, ACTIVE SENTRY® and ACTIVE FLUIDICS TM rapidly detect pressure changes and trigger precise adjustments compensating the occlusion break surge. This is the situation where ocular fluid rushes into the aspiration port after material occluding the phacoemulsification tip clears, filling the vacuum in the tubing and leading to dramatic drops in IOP.
Such pressure drops would have caused the anterior chamber to shallow (decreasing surgical space) (2, 5), or the iris or posterior capsule to move toward the phaco tip, increasing risk of posterior capsule rupture or iris trauma (6, 7).
The combined ACTIVE SENTRY®/ ACTIVE FLUIDICSTM system can be considered comparable to automatic braking systems used in cars. “Just in the same way automatic braking systems respond faster than drivers, the Alcon system responds faster than a surgeon to prevent surge,” says Professor Tognetto. “This is particularly crucial in a university teaching hospital like ours, as trained surgeons feel safer with this machine and appreciate its safety and ease of use. This makes their experience more favorable, and they learn faster.” continues Professor Tognetto.
Benefits of the ACTIVE SENTRY® Handpiece have been demonstrated in a study by Professor Jirásková (Charles University, Prague) who operated on 100 eyes with ACTIVE SENTRY® and 100 with the traditional Centurion Ozil Handpiece (8). Results showed eyes in the ACTIVE SENTRY® group achieved lower IOP (46 mmHg vs 65 mmHg, p<0.005); reduced ultrasound phaco time (30.1 seconds vs 42.2 seconds, p=0,003); reduced cumulative dissipated energy (4.78 vs 6.11 (p=0.002); and eliminated post-occlusion surge.
Professor Paolo Vinciguerra (Humanitas Research Hospital, Milan) agrees that the ACTIVE SENTRY® Handpiece system reduces pain experienced by patients. “It’s really striking when patients who’ve had previous cataract surgery under high IOP have a second operation at lower IOP comment that we must have used a more experienced anesthesiologist,” he says, adding that they explain the anesthesiologist was the same, the only difference was more advanced equipment. “Using lower IOP causes lower mechanical stress to the ciliary body and the zonula. The lower movement of fluids inside the anterior chamber increases safety and reduces biological damage to structures as there is less recycling of liquids and less circulatory damage from the increase in pressure, after 50-55mmHg the central artery stops its blood flow.”
One of the advantages of working under lower IOP is less potential to affect ocular blood flow. An abstract presented by Jing Wang, Kaili Tang, Jinsong Zhang at the Asia-Pacific Association of Cataract and Refractive Surgeons last year, found lower IOP, as opposed to higher IOP, resulted in less ocular hemodynamic parameters variation, and better preservation of macular vessel density (9).
Additionally, there has also been shown to be less damage to corneal endothelium. A study by Taiki Kokubun (Tohoku University, Japan), on patients undergoing cataract surgery to high IOP (50 mmHg) or low IOP (20 mmHg), found four and ninety days after surgery using lower IOP shows statistically significant higher density of the corneal endothelium cells as well as lower central corneal thickness (4).
“When you’re working with the ACTIVE SENTRY® Handpiece everything is under control allowing you to work faster and operate on more cases in a day,” says Vinciguerra. “There are also benefits for the patients. For example, in the glaucomatous patient the use of ACTIVE SENTRY® Handpiece and lower IOP increases the clinical benefit for the patient and the results of the cataract surgery. The cataract surgery becomes safer and easier for the patient.”

Locating the sensor in the ACTIVE SENTRY® Handpiece also eliminates the persistent problem of setting the patient eye level (PEL). The sensor automatically recognizes PEL, eliminating the need for manual adjustments that can result in inaccuracies. Safety can be further enhanced using Alcon’s INTREPID® Hybrid tip, with a rounded polymer edge designed to reduce risk of capsular tears. “This is a great innovation because even if you have surge you can protect the posterior capsule,” says Tognetto.
Despite the advantages of working at lower IOP, many ophthalmologists remain wary of using these settings. A recent survey of 107 ophthalmic surgeons from seven countries, found 48 percent did not think using lower IOP was achievable (3). “One of the greatest concerns of working under lower IOP is not having sufficient anterior chamber space. Surgeons can be astonished to find when they work with the ACTIVE SENTRY® Handpiece and ACTIVE FLUIDICSTM, when inflow and outflow are balanced, that they have sufficient space whatever the pressure,” Tognetto comments.
Ophthalmologists can be reassured that the transition to working at lower IOP can be surprisingly easy. “We find that for experienced surgeons it only takes a few surgeries to become used to working with the ACTIVE SENTRY® Handpiece,” says Professor Tognetto.
References
- Centurion, Vision System with Active Sentry, Handpiece Directions for Use.
- MS Ward, D Georgescu, RJ Olson, " Effect of bottle height and aspiration rate on postocclusion surge in Infiniti and Millennium peristaltic phacoemulsification machines," J Cataract Refract Surg, 34, 1400 (2008).
- Alcon Survey to HCPs 1) Pitcher-Jun-2021, June 2021.
- T Kokubun et al., "Verification for the usefulness of normal tension cataract surgery," Japanese Ophthalmological Society, April 2022.
- M Nejad, VP Injev, KM Miller, "Laboratory analysis of phacoemulsifier compliance and capacity," J Cataract Refract Surg, 38, 2019 (2012).
- IT Tsinopoulos, LP Lamprogiannis, KT Tsaousis, A Mataftsi, C Symeonidis, NT Chalvatzis, SA Dimitrakos, "Surgical outcomes in phacoemulsification after application of a risk stratification system," Clin Ophthalmol, 7, 895 (2013).
- JJ Meyer, AF Kuo, RJ Olson, "The risk of capsular breakage from phacoemulsification needle contact with the lens capsule: a laboratory study," Am J Ophthalmol, 149, 882 (2010).
- N Jirásková et al., "Our experience with Active Sentry and Centurion Ozil handpieces, Czech and Slovak Ophthalmology," 77, 18 (2021).
- J Wang, K Tang, J Zhang, "Effect on Early Ocular Blood Flow after Cataract Surgery with Different Fluidics System in High Myopia Cases," APACRS, ePoster, 2021.
