Many of our patients are light to severe cataract cases. But our team also does a lot of research in the field of premium intraocular lenses, including studies on multifocal, toric, and EDoF intraocular lenses – with which we have a great deal of experience.
We have assessed different IOL types, including Teleon Surgical’s FEMTIS IOL family. When it comes to the Comfort optic, we can clearly show in a laboratory setting and clinical studies that visual acuity results for these lenses at an intermediate distance are quite good. Our published articles have largely focused on lenses with lower add power of 1.5 D, and we were able to show that these lenses not only perform well in the intermediate distance, but they also allow functional visual acuity results in the near distance (1, 2).
Bringing FLACS to the Table
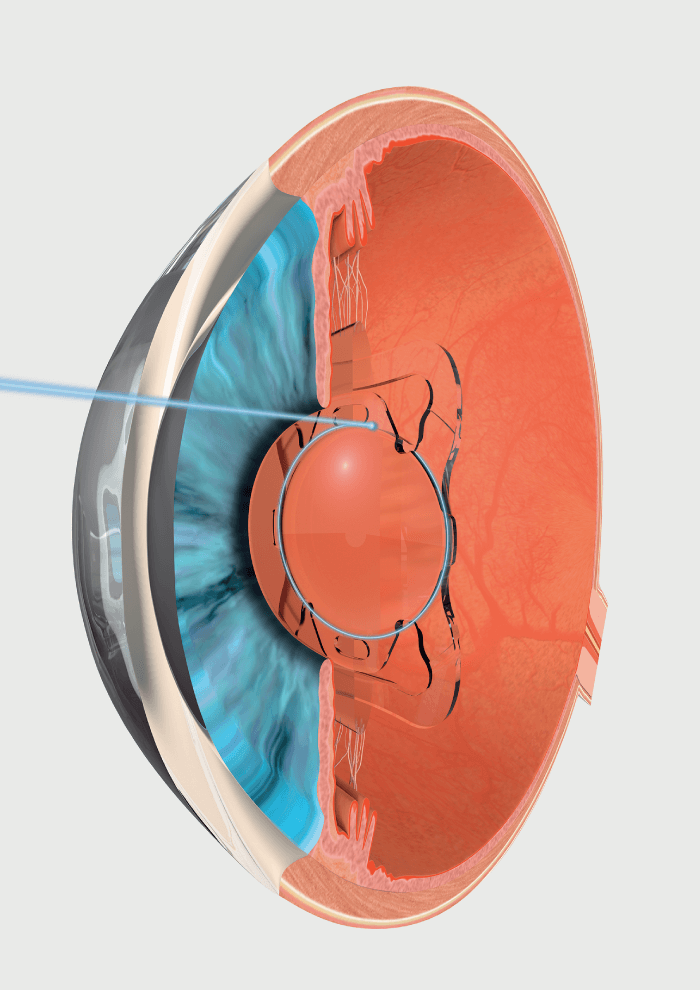
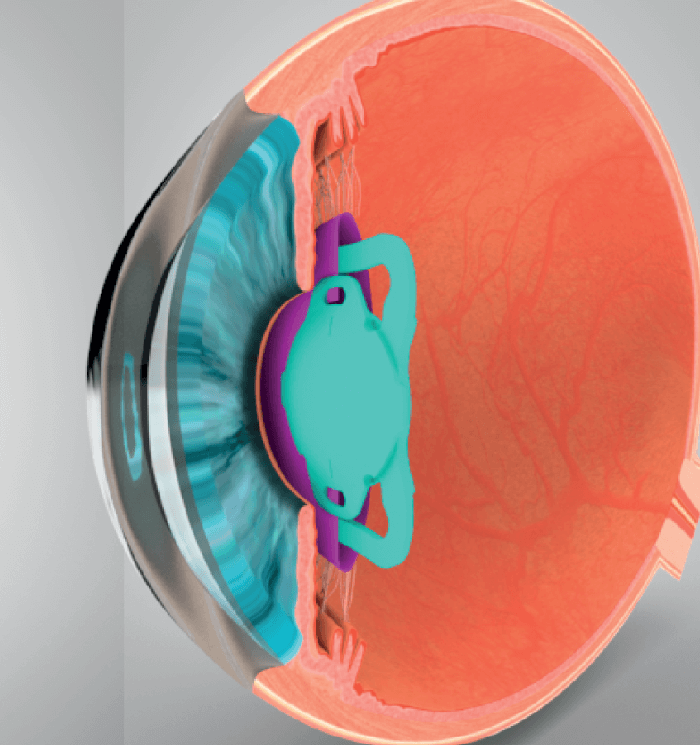
Since the introduction of the system in Europe, our approach has been to offer femtosecond laser assisted cataract surgery (FLACS). In fact, our clinic was one of the first universities in Germany offering FLACS. Personally, I believe FLACS is an extremely precise and great procedure and I often say that it should be made available for many more patients. That said, the real advantages brought by FLACS are currently not maximized when using traditional, widely available plate haptic or c-loop lenses. Why? Because such lenses are implanted in the capsular bag with no further fixation, which might add too little value to the procedure. But with some modern lenses, such as the FEMTIS family of IOLs, surgeons are finally able to take full advantage of FLACS, because the FEMTIS lenses can be placed with highest precision by fixing them in the capsulotomy. Indeed, recent research from a team of experienced surgeons across Germany, the UK, and Spain, proves the point (1). By not just placing these IOLs into the capsular bag like other lenses, but fixing them in the capsulotomy with their four additional clip haptics, excellent outcomes can be realized, including excellent rotational stability and centration.
Now that new ground has been broken, I suspect we will start to see many new developments in the near future, including the introduction of lenses that have been specifically engineered to enhance the benefits of FLACS.
The study using FEMTIS IOLs in FLACS looked at 336 eyes of 183 cataract patients who were followed up for 12 months (1). The IOL was fixated to the anterior capsulotomy. Studied outcomes included UDVA, CDVA, subjective refraction, IOL centration, presence or absence of capsule opacification, and a questionnaire measuring surgeons’ satisfaction with the procedure.
Implantation of the FEMTIS IOL provided excellent visual and stable refractive outcomes and exceptionally high in-the-bag stability over a 12-month period. This lens takes advantage of the high precision and repeatability of capsulotomies created by a femtosecond laser. It can be positioned very predictably and offers an optimal platform for toric, EDoF and multifocal IOL optics.
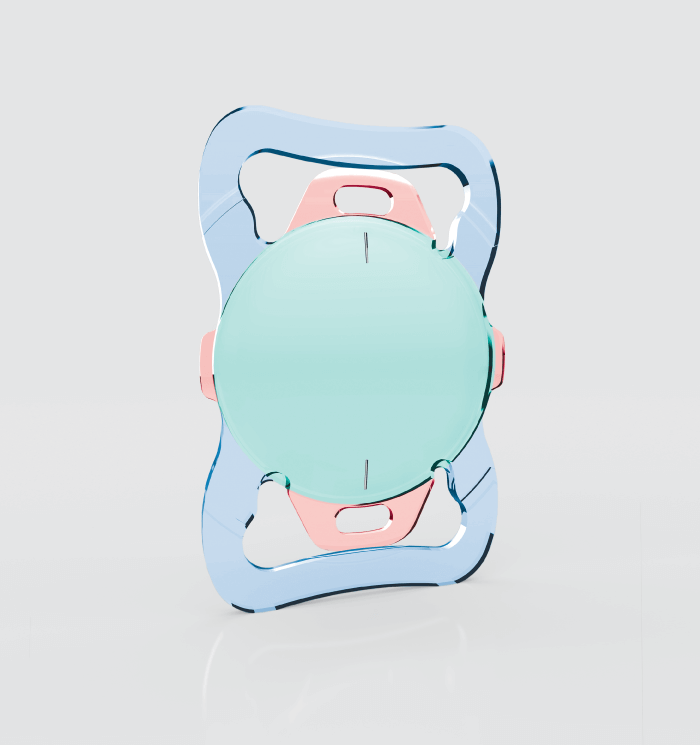
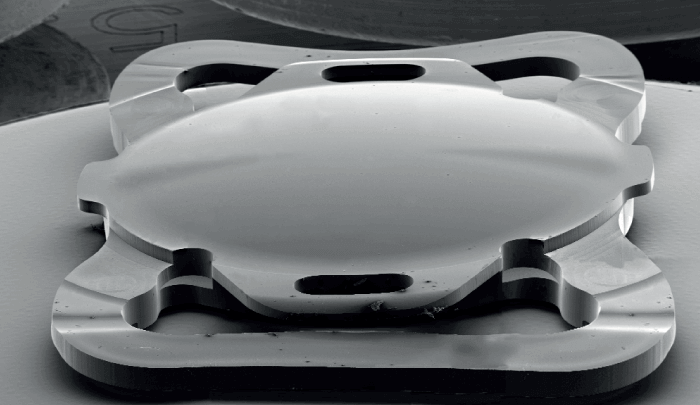
Unique haptic design
The haptic design of the FEMTIS IOL family includes two traditional plate haptics plus another four smaller clip haptics. These smaller haptics are anteriorly based and are used to align the lens into the capsulotomy, holding the lens in the right position. When the lens is fixated in the capsulotomy, the surgeon can be sure that the lens is perfectly centered and in axis in case a toric lens was used. Of course, centration is especially important when considering multifocal or toric lenses, as well as aspheric lenses, especially aberration correcting IOLs.
In FLACS with the FEMTIS lens, the IOL is placed exactly where you want it to be – and, crucially, with a very low risk of rotation and decentration. I am sure I am not alone in fully appreciating such consistency.
All about outcomes… and satisfaction
My patients are very satisfied with the FEMTIS and FLACS combination. When it comes to the FEMTIS family, the difference is really measured in terms of high surgery success rates and the previously mentioned lower risk of decentration and rotation. In terms of surgeon experience, there is a small learning curve to get familiar with incubating four additional haptics, which is covered by a small amount of training; however, most surgeons involved in our study became quickly familiar with the modified approach.
Patient selection
Our recent study on the outcomes of the FEMTIS IOL used after FLACS (1) had a typical design, so only relatively healthy patients were included. But now that I have had more experience with the FEMTIS lenses, I would say that there are very few candidates who are not suitable for the procedure, especially taking into account that FEMTIS is available as monofocal, EDoF and multifocal, as well as toric IOL model. In that low percentage, I would include patients who suffered complications during capsulotomy or capsulorhexis, such as radial tears. There are also very rare cases when a patient's pupil is too small for successful surgery. And if candidates have very loose zonules, I would be hesitant to operate due to the additional manipulation during haptic incubation into the capsulotomy. Other comorbidities should not be a problem, as long as the capsulotomy is properly done and the lenses and zonules are stable enough.
What surgeons should know
When implanting these intraocular lenses, make sure you first remove the viscoelastic from behind the lens. Once the lens is incubated into the capsulotomy, it’s rather difficult to go behind to remove the viscoelastic material. I would advise surgeons to start with the enhanced monofocal version of the lens to build familiarity with the procedure; once you’re familiar with the extra haptics, you can graduate to the EDoF, multifocal and toric versions!
References
- FTA Kretz et al., “Clinical evaluation of functional vision of +1.5 diopters near addition, aspheric, rotational asymmetric multifocal intraocular lens,” Korean J Ophthalmol, 30, 382 (2016). PMID: 27729759.
- TM Yildrim et al., “[In vitro evaluation of the optical quality of segmental refractive multifocal intraocular lenses],” Klin Monbl Augenheilkd, 236, 983 (2019). PMID: 29117609.
