- To save pediatric patients the stress of multiple interventions, the ideal surgical approach should adequately lower IOP in a single procedure when successful – and guide subsequent therapeutic strategy when unsuccessful
- Procedures such as goniotomy treat only a portion of the angle; reliance on such techniques may require repeated angle procedures to achieve the desired IOP lowering effect. To perform a goniotomy, good visualization of the angle structures is necessary and this can be an issue when children present with significant corneal clouding
- The 360° trabeculotomy, by contrast, treats the entire angle at once. If this procedure is not effective in controlling the IOP, traditional glaucoma surgery (filtering surgery or glaucoma drainage device surgery) is needed
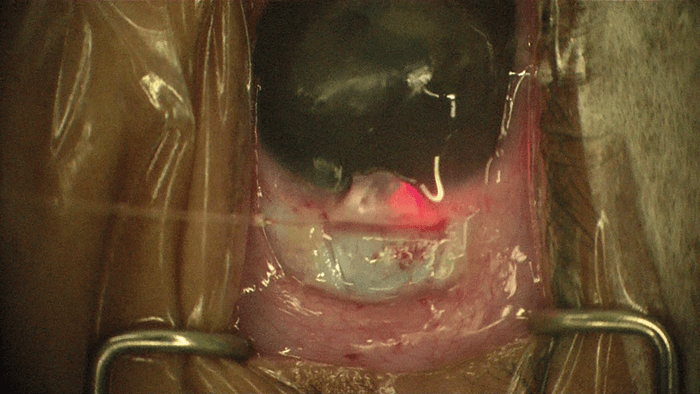
- Illuminated devices (visible through the sclera as they are pushed around Schlemm’s canal) help the surgeon guide the catheter during the 360° trabeculotomy procedure, irrespective of corneal opacity.
- To save pediatric patients the stress of multiple interventions, the ideal surgical approach should adequately lower IOP in a single procedure when successful – and guide subsequent therapeutic strategy when unsuccessful
- Procedures such as goniotomy treat only a portion of the angle; reliance on such techniques may require repeated angle procedures to achieve the desired IOP lowering effect. To perform a goniotomy, good visualization of the angle structures is necessary and this can be an issue when children present with significant corneal clouding
- The 360° trabeculotomy, by contrast, treats the entire angle at once. If this procedure is not effective in controlling the IOP, traditional glaucoma surgery (filtering surgery or glaucoma drainage device surgery) is needed
- Illuminated devices (visible through the sclera as they are pushed around Schlemm’s canal) help the surgeon guide the catheter during the 360° trabeculotomy procedure, irrespective of corneal opacity.
Treating children with congenital glaucoma is often a considerable challenge. Early detection and timely intervention are essential to achieving successful outcomes. These children can present with severely elevated IOP, and if untreated, the natural course is rapid progression to blindness from optic nerve damage. Another significant contributor to vision loss is dense amblyopia from anisometropia or corneal opacification. Surgical options had typically been limited to goniotomy and trabeculotomy with either a Harms trabeculotome or suture, but the 360° trabeculotomy with an illuminated microcatheter, performed via an ab-interno or ab-externo approach, is gaining increased popularity. The main advantage of this approach is that it allows the surgeon to treat the entire angle in a single procedure with anatomic visualization of the catheter. Since the pathology is usually limited to the entrance into the drainage system, gaining access to Schlemm’s canal can successfully fix the problem in many cases. Though the entire angle does not necessarily have to be treated each time to have a successful outcome, a full 360° treatment likely enhances the chances of success. I have had numerous cases where we started with a nasal goniotomy and then moved on to a temporal trabeculotomy, and in some cases went back a third time into the angle to try a more extensive goniotomy.
Another advantage of the 360° trabeculotomy is that the procedure leaves no question as to whether additional angle surgery is needed. If the IOP becomes elevated again, then the presumption is that these children have pathology in the downstream collector channels and need traditional glaucoma surgery, either a trabeculectomy or tube shunt surgery. Thus, a major benefit of doing the 360° trabeculotomy first is that a decision can be made sooner to proceed to traditional glaucoma surgery if initial angle surgery is not successful. The last benefit of a 360° trabeculotomy from an ab-externo approach is that it can be performed regardless of how well the angle can be viewed. Elevated IOP in children with congenital glaucoma often leads to significant corneal edema and haze, which obscures the surgeon’s direct view of the angle when attempting to perform a goniotomy or even the gonioscopy-assisted transluminal trabeculotomy (GATT) procedure.
Congenital glaucoma is rare, and thus mastering various angle-based surgeries is difficult. Due to the many advantages of an ab-externo 360° trabeculotomy, it makes sense to learn this procedure and be prepared to use it as the first intervention for congenital glaucoma cases.
Breaking into Schlemm’s Canal
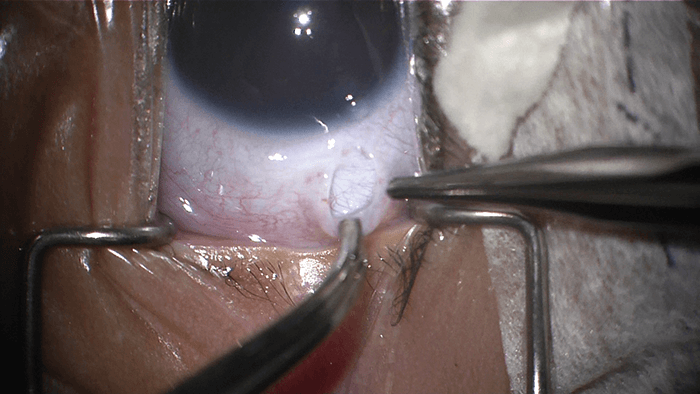
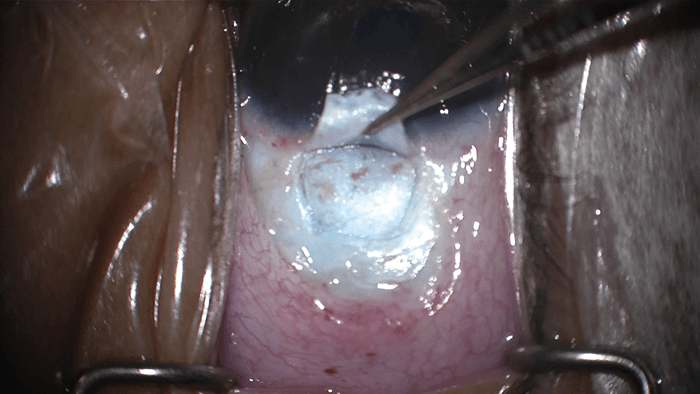
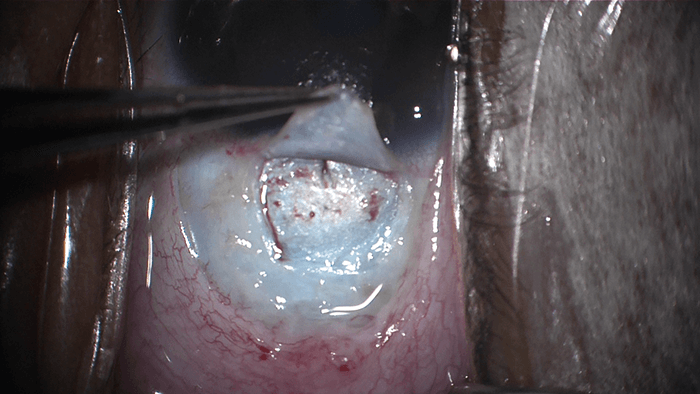
I start with a temporal conjunctival peritomy (spare the superior conjunctiva), which gives me access to the sclera (Figure 1). The next step is to make a scleral flap of your choice (Figure 2); I prefer a 3.5 × 3.0 mm trapezoidal flap as I do for my trabeculectomy. Maintaining depth here is key (90 percent depth if possible). I then make a scratch-down incision with a #75 blade to “un-roof” Schlemm’s canal (Figure 3). Picking the right spot is a challenge as the limbal anatomy in these children is often distorted due to the large size of the eye. There are landmarks that can help you locate Schlemm’s canal, as well as distinct patterns in the orientation of the scleral fibers to help guide the surgeon, but often a certain feel is required. I’ll admit it’s not very scientific but you will know you’ve found the correct spot once you see an egress of fluid or blood. During this procedure, you should take great care to avoid penetrating the anterior chamber (AC) as this can lead to collapse of the canal and increases the difficulty of threading Schlemm’s canal. The key to un-roofing Schlemm’s canal is to go slowly. You can always continue deeper with your dissection but you cannot go back once you have entered the AC.Are you where you think you are?
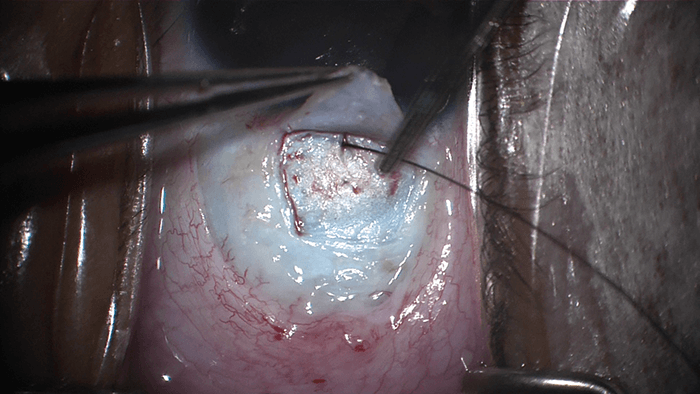
At this stage, I insert a 6-0 nylon suture into the canal to ensure that I’m not in a false channel (Figure 4). If the nylon suture passes through freely, you can be reasonably sure you’re in the right spot. In the past, you would have to pass a suture blindly around the entire canal and it would be difficult to tell if one veered off into a collector channel or into the suprachoroidal space. The illuminated microcatheter allows the surgeon to see the exact location of the probe tip as it is being advanced (Figure 5). Many surgeons would agree that the canal “likes the catheter” and it can be advanced smoothly. If the catheter encounters resistance, cohesive viscoelastic can be injected through the catheter tip to dilate the canal and release possible adhesions inthe area.
Tying up loose ends
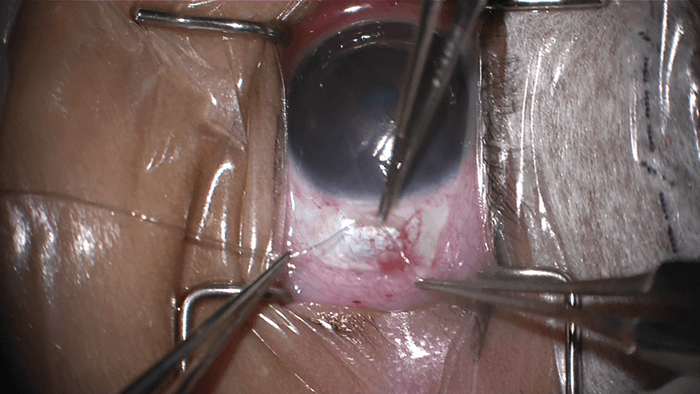
Once you have passed your device around the canal and back out again, you grab both ends and pull (Figure 6). The angle is now open and a cleft is created, exposing the inner wall of Schlemm’s canal. If possible, leave a strip of tissue in place where you made the scratch-down incision to allow for easier closure of this site. This can be achieved by releasing one end of the catheter at the very end as you pull through. We then close the scleral flap and the conjunctiva – and that’s it! Though the keys to surgical success have been outlined above, the first step in treating these children is to make the correct diagnosis. An examination under anesthesia (EUA) is almost always required, since a thorough examination in the office is often not possible. A complete examination includes: IOP check (Tonopen and/or Perkins Tonometer readings) at the time of anesthesia induction, slit-lamp examination of the anterior segment, measurement of corneal diameter and central corneal thickness, gonioscopic evaluation of the angle, axial length measurement, optic nerve examination, and dilated funduscopic examination. Once examination is complete and the diagnosis of glaucoma is made, the surgeon must decide whether or not surgical intervention is appropriate. In most cases of childhood glaucoma, surgery is required. I always have a thorough discussion in the office prior to the EUA about the risks, benefits, and alternatives, to the potential surgical procedure as that is the best time for the parents to ask questions and gain a better understanding of what we hope to achieve. After the EUA, I review my findings with the family and emphasize my recommendation to proceed with same day surgery to prevent additional trips to the operating room. As discussed, the 360° trabeculotomy via an ab-externo approach is my first option. If the IOP is not controlled after this procedure, I proceed to either tube shunt surgery or trabeculectomy. Though both trabeculectomy and tube shunt surgery have evolved tremendously over the years with advances in surgical technique and improved methods to modulate wound healing, they remain difficult to perform in the pediatric population and carry significant long-term risk.Pediatric glaucoma is not the easiest condition to treat, but providing care to children with glaucoma is always rewarding. These children can go on to live a life with their full visual potential. Joseph Panarelli specializes in the treatment of adult and pediatric glaucoma. He currently serves as the Associate Residency Program Director and Glaucoma Fellowship Director at the New York Eye and Ear Infirmary of Mount Sinai. He received his undergraduate and medical education from Georgetown University and began his postdoctoral education at the Lenox Hill Hospital with a general medicine internship. He then completed his ophthalmology residency at the New York Eye and Ear Infirmary and his glaucoma fellowship at the Bascom Palmer Eye Institute in Miami, FL. To view the video online, visit top.txp.to/issues/0717/501
