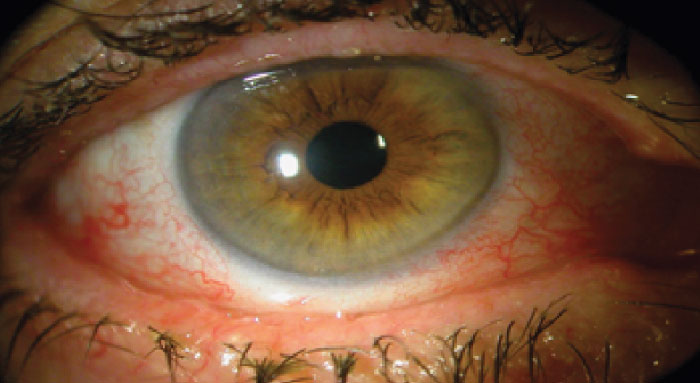
It is estimated that 100 million people are affected by dry eye globally. These individuals make up a large portion of the ophthalmic patient population, presenting with irritation, discomfort, light sensitivity, and fluctuating vision. But despite our best efforts, there are some who experience little to no improvement in their symptoms – even after maximum medical intervention. Dry eye patients who do not respond to treatment may be suffering from a second condition: conjunctivochalasis (CCh). CCh is caused by the degeneration of the Tenon’s capsule – a result of high matrix metalloproteinase activity. The unhealthy Tenon’s causes the conjunctiva to loosen, creating folds that interfere with the tear meniscus, prevent tear clearance, and diminish the volume of the fornix. Over time, the loose conjunctiva continues to contract – shortening the fornix and further diminishing its ability to replenish the tear meniscus sufficiently. Orbital fat prolapse can further compound the problem.
Previous surgical interventions have focused on eliminating folds by removing part of the conjunctiva – but this is only a temporary solution. Though conjunctiva removal alone offers some relief, it runs the risk of further diminishing the tear reservoir – and it does little to prevent fat prolapse. So what’s the solution? Enter the Reservoir Restoration (RR) procedure using AmnioGraft cryopreserved amniotic membrane from Bio-Tissue. Using AmnioGraft to recreate a smooth ocular surface, the procedure helps provide a platform for regenerative healing. By reconstructing the inferior fornix this way, RR re-establishes the normal anatomical tear reservoir – fixing the eye’s inability to hold fluid – and thus delivers superior results for patients.
Arla Genstler – an ophthalmologist and owner of Genstler Eye Center, who regularly uses the procedure in her practice – can attest to such results. “The RR method offers unparalleled benefits: improved tear drainage, restored normal anatomy and blinking, and reservoir capacity. This restored mechanical function is what provides the symptomatic relief that the patient experiences.”
“From a surgical point of view, the procedure is relatively straightforward. One has to be cognizant of anatomy – you are resecting orbital fat around the ocular muscles, after all – but, it is a procedure with good visualization,” says Genstler. “When a patient has tried multiple modalities with limited success, they are grateful to have a procedure that offers immediate and lasting relief. It’s great that we can provide a definitive solution.”
But, as with all procedures, postoperative outcomes rely on preoperative planning – and that includes effective patient communication. “It is important to stress that the procedure only addresses one component of a multifactorial disease,” says Genstler. “It is not a cure-for-all, it simply addresses the mechanical issue. And so, if a patient has Meibomian gland dysfunction or aqueous deficiency, they will still have those same conditions after the procedure. By educating the patient ahead of time, you can set realistic expectations.”
The procedure is gaining in popularity. And Genstler is keen to spread the word further; her practice has put on several roundtable discussions with optometric colleagues to increase their awareness of the RR procedure as a potential treatment for CCh. “It offers another means of addressing the pathology of the ocular surface disease, with benefits beyond symptomatic relief. We can offer increased quality of life – allowing patients to enjoy activities like reading without the constant feeling of something in their eye,” says Genstler. “And that is priceless.”
Reservoir Restoration 101, with Arla Genstler
CCh is becoming increasingly common, particularly among young people; I suspect this has something to do with the increase in inflammatory mediators from our diet and the marked increase in computer device usage. In any case, the only procedure that I have used to treat CCh is RR. Why? For one, I do not like any procedure that shortens the inferior cul-de-sac. Instead, I believe we need to perform a full reconstruction and restore normal anatomy to offer benefits to the patient.
I use The RR Method (see below) to reconstruct the reservoir. In short, I remove the degenerated Tenon’s, resect some of the anterior orbital fat, and then place a layer of amniotic membrane deep into the surgical site. The process works beautifully – the tear meniscus returns, the staining of the lid margin resolves, and the patient enjoys an uninterrupted blink.
The RR procedure is a wonderful addition to the armamentarium of ocular surface disease treatments. I would encourage anybody with a comprehensive ophthalmology practice to add RR to their skillset – particularly those with a surgical emphasis, where the ocular surface is crucial to pre-operative measurements and post-operative outcomes.

The Reservoir Restoration Procedure - Surgical Steps
1. Apply 2 percent lidocaine gel
2. Place a 7/0 Vicryl corneal traction suture
3. Inject (2 percent) lidocaine with (1/10,000) Epinephrine sub-conjunctiva in the area to be dissected
4. Start your incision with a relaxing incision at the outside edge of the dissection
5. Begin a peritomy 1-2 mm from limbus taking care to preserve the limbal stem cells
6. Trim about 1-2 mm of conjunctiva (enough to recess its edge into the fornix)
7. Aggressively dissect and remove all abnormal Tenon’s fascia from the episcleral surface
8. Cauterize prolapsed orbital fat to further deepen the fornix
9. Cauterize the leading edge of Tenon’s and prolapsed fat
10. Cut and glue down a small piece of AmnioGraft® to cover the area of the rectus muscle insertion (This will replace Tenon’s and prevent muscle restriction) (Figure 2)
11. Cut and glue down a larger piece of AmnioGraft® to cover the entire surgical site. (Figure 3). In the fornix push tissue up against the edge of the Tenon’s and over the edge of the conjunctiva (Figure 4)
12. Make sure edges other than in fornix are covered by 1 mm of conjunctiva
13. Glue down the small flap of conjunctiva at limbus
14. Check edges of conjunctiva to be sure they are glued down
15. Remove all excess glue
16. Remove traction suture
17. Place bandage lens on cornea
