Haroon Ilyas, MD, is an ophthalmic surgeon at Brandon Eye Associates - a comprehensive ophthalmology practice in Brandon, Florida, USA. Dr. Ilyas has been treating acquired ptosis in adult patients with Upneeq® (oxymetazoline hydrochloride ophthalmic solution), 0.1% a novel, non-surgical therapy from RVL Pharmaceuticals that received FDA approval in 2020. In this article, he explains how Upneeq works within his practice and how it has changed his diagnosis and treatment protocols.
The “before” times
Prior to Upneeq’s approval, the status quo of diagnosing and treating patients with ptosis was most often to leave the problem unaddressed unless the patient complained or the condition was causing obvious impairment (1). Although patients may have cosmetic anxiety over their appearance, many assume that if their physician hasn’t addressed the ptosis, it is not severe enough to warrant attention, let alone treatment. Additionally, until recently, the primary ptosis treatment available to me was surgical, so patients exhibited some reluctance, as did I.
Keeping good time
The timely detection and intervention of ptosis can minimize the duration of cosmetic and visual function consequences (2). It’s also important to keep in mind that ptosis may be associated with neurologic or orbital diseases and consideration should be given to these conditions during diagnosis. Early to middle stages of acquired ptosis typically involve cosmetic concerns, with eyes appearing bored or sleepy; sometimes, there is asymmetry between ptosis levels in each eye. Late stages typically bring about more medical symptoms, including visual impairment, eye strain, brow ache, neck strain, and fatigue (although some of these may occur even in earlier stages). These symptoms can drastically affect my patients’ daily living and therefore quality of life – activities such as watching TV, reading, or fine manual work can become much more difficult.
In its early stages, acquired ptosis may be confused with dry eye; presenting a diagnostic challenge. Due to dry eye’s pervasiveness and shared symptoms of visual strain and fatigue, clinicians may misdiagnose ptosis complaints as dry eye and throw artificial tears and other dry eye therapies at the problem. This can lead to patients developing visual symptoms from their acquired ptosis in the more moderate to severe stages. Like with most ocular diseases, addressing ptosis as early as possible may avoid more significant symptoms. Clinicians may also appreciate the fact that acquired ptosis is a medical condition and addressing it may increase the overall complexity of the visit, while addressing the root of their patients’ problems.
Talking about ptosis
Upneeq’s ready availability has renewed my interest in finding acquired ptosis and treating it without surgery. Its accessibility has also made it much easier to discuss acquired ptosis with patients, and I have found that almost all patients are grateful to me for bringing awareness to the issue, explaining their symptoms, and acknowledging their cosmetic concerns. Because Upneeq often starts working within fifteen minutes of application, I will often trial it with patients on the spot so they can see the results for themselves. I also get them to take a selfie before the treatment (in which I ensure that they don’t raise their brows to “hide” the ptosis) and a follow-up selfie an hour later to see the impact. Seeing is believing, of course, so I think that providing the patient a sample is important so that both the physician and the patient can see how the treatment worked for the patient. When I prescribe Upneeq I also make sure to tell my patients that they may have some adverse reactions and that in the clinical trials, the most common treatment emergent adverse reactions which occurred with an incidence 1 to 5% were: punctate keratitis, conjunctival hyperemia, dry eye, blurred vision, instillation site pain, eye irritation and headache.
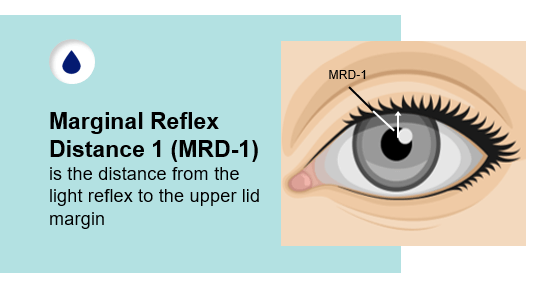
Since prescribing Upneeq, I have started routinely taking MRD1 recordings in patients with acquired ptosis. This acts as a data point for both diagnosis and tracking progression of acquired ptosis. I now also pay much more attention to the possibility of acquired ptosis when I hear about fatigue or eye strain before offering lubricant eye drops. Upneeq has become my first-line treatment of acquired ptosis in adult patients who are candidates for the drop. It’s important to keep in mind that Upneeq may not be right for all patients. Since Upneeq may impact blood pressure, I think physicians should tell patients with cardiovascular disease, orthostatic hypotension, and/or uncontrolled hypertension or hypotension to monitor their condition and call the clinic if it worsens.
Interestingly, my oculoplastic colleague was concerned that Upneeq would reduce the number of consultations she received. Contrary to this, her consultations have actually increased because of the practice’s and patients’ greater awareness of acquired ptosis – highlighting the importance of that awareness and its benefits for comprehensive practices.
Distribution and pricing
From a physician standpoint, the product’s distribution model is the simplest I’ve seen in my career to date – mostly because it works outside of an insurance model. After I recommend it to a patient, my scribe sends the prescription to RVL Pharmacy and the company contacts the patient to ship it out to them directly. That’s it; there’s no insurance and no callbacks for the physician. The great thing is that after diagnosing, discussing, prescribing, and treating with Upneeq, the patient takes over. If they are satisfied with their results, they order direct from RVL Pharmacy and we’ve had zero callbacks to our office – truly the first eye drop about which I can make that statement. Because it’s a direct-to-patient billing model, it has been one of the few products that I enjoy prescribing because of the hands-off approach from a physician perspective after writing the prescription.
The ultimate cost of the medication depends entirely on the patient – not only their financial circumstances, but how they weigh the expense against the perceived benefit. Upneeq is indicated for daily use, however patients have ownership over how often they use the product. For example, I have many “weekend warrior” patients with ptosis who use the product when they plan to see other people and want to make their eyes look more open, but I also have patients who use the drop every day. Fortunately, the product comes in unit dose preservative free vials which allows people to work out a system of Upneeq treatment that best suits them, and overall, I think the price is very reasonable. We also make sure to instruct patients to not touch the tip of the container to their eye or any other surface to avoid contamination.
Positive results
In my experience, Upneeq works on both a functional and cosmetic level for patients with visual impairment symptoms from acquired ptosis – and many patients are happy with their results. I’ve been pleased with the outcomes for acquired ptosis patients in my practice, including patients with late-stage acquired ptosis.
For cataract patients going for premium lenses with diffractive technology, the amount of light coming into the eye makes a difference. Some of these patients also have acquired ptosis and addressing their eyelid position may improve vision (especially in lower light conditions). I had one patient in particular who had fairly significant cataracts and noticeably asymmetrical acquired ptosis between her eyes. Following her use of Upneeq, she was thrilled with the results – to the point where, after her successful cataract surgery (20/20 in both eyes), she talked about the improvement in the appearance of her eyelids as much as she did about her vision. It really shows how concerned patients can be about ptosis and the significance of now having a nonsurgical option.
Haroon Ilyas is a paid consultant of RVL Pharmaceuticals, Inc.
IMPORTANT SAFETY INFORMATION
INDICATION
UPNEEQTM (oxymetazoline hydrochloride ophthalmic solution), 0.1% is indicated for the treatment of acquired blepharoptosis in adults.
WARNINGS AND PRECAUTIONS
• Ptosis may be associated with neurologic or orbital diseases such as stroke and/or cerebral aneurysm, Horner syndrome, myasthenia gravis, external ophthalmoplegia, orbital infection and orbital masses. Consideration should be given to these conditions in the presence of ptosis with decreased levator muscle function and/or other neurologic signs.
• Alpha-adrenergic agonists as a class may impact blood pressure. Advise UPNEEQ patients with cardiovascular disease, orthostatic hypotension, and/or uncontrolled hypertension or hypotension to seek medical care if their condition worsens.
• Use UPNEEQ with caution in patients with cerebral or coronary insufficiency or Sjögren’s syndrome. Advise patients to seek medical care if signs and symptoms of potentiation of vascular insufficiency develop.
• UPNEEQ may increase the risk of angle closure glaucoma in patients with untreated narrow-angle glaucoma. Advise patients to seek immediate medical care if signs and symptoms of acute narrowangle glaucoma develop.
• Patients should not touch the tip of the single patient-use container to their eye or to any surface, in order to avoid eye injury or contamination of the solution.
ADVERSE REACTIONS
Adverse reactions that occurred in 1-5% of subjects treated with UPNEEQ were punctate keratitis, conjunctival hyperemia, dry eye, blurred vision, instillation site pain, eye irritation and headache.
DRUG INTERACTIONS
• Alpha-adrenergic agonists, as a class, may impact blood pressure. Caution in using drugs such as beta-blockers, anti-hypertensives, and/or cardiac glycosides is advised. Caution should also be exercised in patients receiving alpha adrenergic receptor antagonists such as in the treatment of cardiovascular disease, or benign prostatic hypertrophy.
• Caution is advised in patients taking monoamine oxidase inhibitors which can affect the metabolism and uptake of circulating amines.
©2021 RVL Pharmaceuticals, Inc. All rights reserved.
Upneeq® is a registered trademark of RVL Pharmaceuticals, Inc
PM-US-UPN-0496
References
- J Bacharach et al., “A review of acquired blepharoptosis: prevalence, diagnosis, and current treatment options,” Eye (Lond) [Online ahead of print] (2021). PMID: 33927356.
- Y Wang et al., “Incidence and risk of ptosis following ocular surgery: a systematic review and meta-analysis,” Graefes Arch Clin Exp Ophthalmol, 257, 394 (2018). PMID: 30203103.
