The evolution of femtosecond laser-assisted cataract surgery (FLACS) has been accelerating since Zoltan Nagy performed the first anterior capsulotomy in humans with a femtosecond laser as part of cataract surgery in 2008. Even the original smartphone is older – Apple launched the first iPhone in 2007, and since then, both products have improved beyond what could have been imagined back then. But it’s not the smartphone that is giving people a glimpse at the future today; it’s lasers like the LENSAR with Streamline Laser System.
The LENSAR with Streamline is expressly designed for refractive cataract surgery, and it brings what was tomorrow’s features to today’s refractive cataract surgeons. It is the first cataract laser system to enable automation of key surgical elements with the introduction of multiple new applications:
• Wireless integration with the Cassini Corneal Shape Analyzer
- Other topographers, including the Topcon Aladdin biometer, are being evaluated
• Astigmatism Management
- Arcuate incision planning
- Steep axis corneal marks
• Automatic cataract density imaging
• Automatic fragmentation patterns
We spoke with three eminent refractive cataract surgeons about their experience with LENSAR with Streamline, and how it can help improve not only patient satisfaction, but also provide excellent clinical outcomes.
Rob Morris
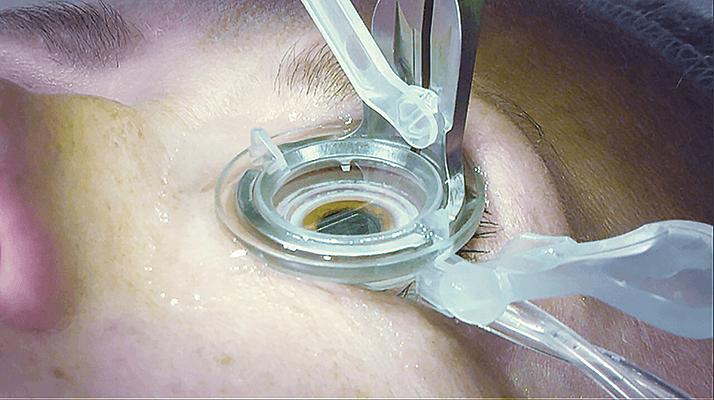
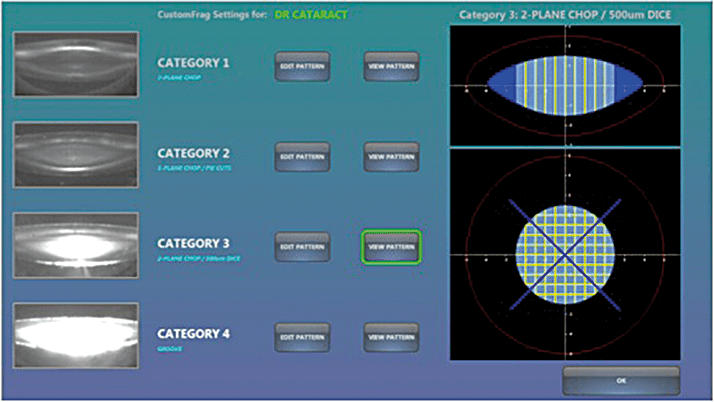
Medical Director and Consultant Ophthalmic Surgeon Optegra Eye Health Care, UK When Charlie Kelman began doing phacoemulsification in the late 1970s, he was told it would never work. I started doing it 20 years later, and a lot of surgeons still said things like, “This will never take off in my hands,” or, “In my hands, extracapsular surgery is just as good” – and look where phaco is now. New technology is always difficult to introduce, and often, the barrier to widespread uptake is cost. Technology is expensive and it takes a while to refine it and to gather enough evidence to prove its benefits. I think the adoption of FLACS is similar and the LENSAR with Streamline is going to take FLACS to the next level. One issue with standard laser capsulotomies is that it’s performed slowly – microsaccades can mean that the laser can’t perforate accurately. With the LENSAR laser, the capsulotomy can take less than two seconds giving tight perforations and virtually no tears. It is technology advances like these that will level the playing field on surgical skills and encourage more ophthalmologists to use FLACS. A workflow solution that meets your practice’s needs Convenience helps, too; the LENSAR laser has a small enough platform to be kept in the operating room, so that the patient doesn’t have to be moved from one place to another. It also does not have a fixed bed, so if you have a patient under sedation, you can just swing the laser over without having to reposition them. And of course, the final major factor is cost. In the Optegra business model, the patient pays a fixed price for clear lens extraction regardless of which devices are used and what lens is implanted. So the LENSAR laser is an attractive option in that it has a faster and more convenient workflow, which should appeal to any surgeon considering a move to femto-phaco. A solution tailored to your patient’s cataract A big advantage of the LENSAR laser is that its patient interface (Figure 1) requires minimal pressure to be applied to the cornea. It’s a fluid-based system with low suction pressure, so there is little or no risk of central retinal artery occlusion and the patient can still see. But best of all, prior to treatment, the system takes up to 16 scans and reconstructs them into a detailed 3D image that can be used for extensive treatment planning including automatically optimizing the fragmentation based on the cataract density. The way OCT based lasers work is that the surgeon sets up fragmentation patterns prior to the procedure without any customization based on cataract density.LENSAR with Streamline uses Scheimpflug imaging to visualize the cataract in enough detail to allow automatic classification of the cataract density; then, the device can set up the surgeon’s pre-selected fragmentation pattern for the appropriate cataract density even allowing for the automatic isolation of fragmentation to the nucleus (Figure 2). Just like we wouldn’t put unnecessary phaco energy where it wasn’t needed, instead of universally applying a burst of laser energy to the entire lens volume, the LENSAR with Streamline will customize the fragmentation appropriately to each individual cataract, saving both time and energy.
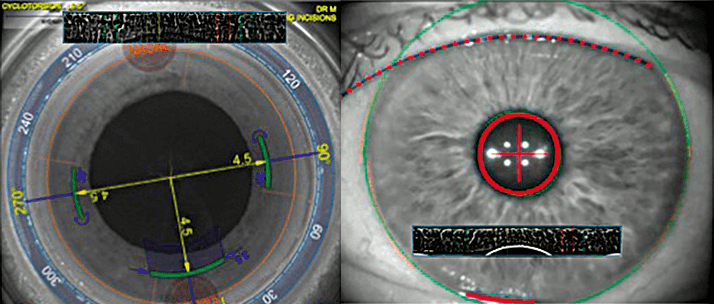
Iris registration I think what’s really going to set LENSAR with Streamline apart is the fact that it’s the only femtosecond laser with iris registration technology (Figure 3). I think it’s a key advantage because I have so many patients whose trickiest issue is astigmatism. The iris registration feature allows for automatic adjustment for cyclorotation that vastly improves incision accuracy versus ink marking the eye. Sometimes patients have a small amount of astigmatism – a diopter or so – and the patient or the surgeon may not want to use a toric IOL. Streamline lets me address that – I can treat the astigmatism at the time of surgery by planning arcuate incisions along with the cataract procedure.
Unparalleled accuracy LENSAR with Streamline is great for increasing accuracy and reducing error too, because Streamline includes wireless communication with the laser to automatically populate key patient data from the Cassini. That means you minimize the risk of treating the wrong axis, and you can’t make manual errors in transcription. The British cycling coach Dave Brailsford gave a very good analogy for cycling which I think is applicable for FLACS; he said that if you strip a bike down and rebuild it with a marginal improvement to each part, the overall improvement is significant: the philosophy of marginal gains. All of these improvements to cataract and refractive surgery are marginal gains, like the parts of a bicycle, but I think there are a lot of those gains to be made using LENSAR with Streamline, and they add up to a very big step forward indeed.
Robert J. Weinstock
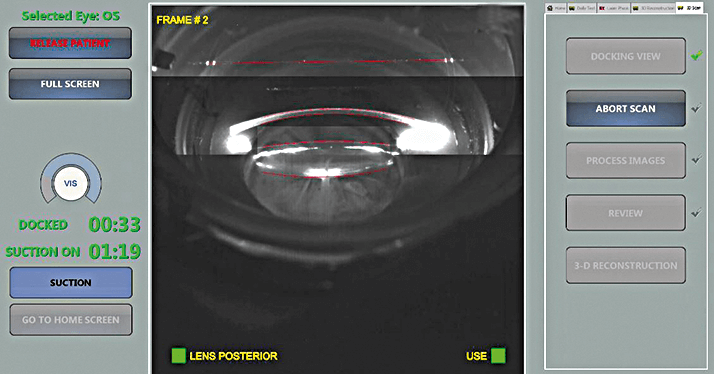
Ophthalmologist, The Eye Institute of West Florida, Largo, FL, USAAssistant Clinical Professor, University of South Florida, Tampa, FL, USA With the recent release of Streamline, the LENSAR laser has a range of new features for surgeons – wireless integration with Cassini, iris registration, astigmatism treatment planning, steep axis corneal marks, automatic cataract density imaging, and automated lens fragmentation patterns. Most impactful among these in my view are the improvements to astigmatism management using the laser. A speedier workflow Until now, we’ve had to do corneal ink marking to align the laser and the primary meridians of the cornea. But with the new software, we can perform iris registration based on a preoperative image taken by the Cassini Corneal Shape Analyzer and wirelessly feed that information directly to the laser. The Cassini verifies image compatibility at the point of capture to minimize the risk of cyclorotation compensation failure once the patient is already in the operating room. Streamline corrects for cyclorotation after docking to the laser using iris architecture details from the Cassini image, this means that the surgeon does not need to visually verify that cyclorotation compensation was accurate, as is the case in some vessel-based tracking systems. The automated data transfer reduces procedure time and complexity, eliminates transcription errors, and allows surgical staff to focus on the procedure itself rather than on moving data between devices. Efficiency and automation for excellent outcomes After the patient is docked under the laser and iris architecture details are registered, multiple astigmatism management techniques are available such as arcuate incisions or steep axis corneal marks that a surgeon may use to guide toric IOL placement. The benefit of using the laser to manage astigmatism is that I am confident that the treatment is at the appropriate axis – unlike manual ink marks. No matter how well astigmatism correction works, it won’t give us a good result if it’s not at the right axis. Streamline has built-in arcuate incision planning tables where surgeons can enter a surgically induced astigmatism measurement and a nomogram of their own calculation. The software will automatically account for that and plan corresponding arcuate incision locations, depths and lengths, or corneal steep axis marks. It also corrects for cyclotorsion by comparing a preoperative iris image to the dilated iris after the eye is docked. That’s unique to Streamline – no other laser system compensates for cyclotorsion after docking the eye to the laser, thus minimizing the potential for changes caused by the docking process itself (Figure 1). Having all that surgical planning automated is also a big time saver, as well as reducing the risk of calculation errors, so it’s a major improvement in the astigmatism management component of laser cataract surgery. Look into more precise treatment I noticed early on that LENSAR with Streamline’s Scheimpflug imaging system (Figure 4) gave me a very different look at the anterior segment of the eye compared to the OCT imaging systems of other lasers. OCT doesn’t pick up on cataract density as well as Scheimpflug imaging – but it’s important information, because a denser cataract might call for more robust fragmentation. Streamline classifies the cataract based on its density and then recommends an appropriate laser fragmentation pattern. Those automated fragmentation patterns are based on parameters that I programmed when the Streamline was first installed on my laser. Once the automated patterns were set up, I didn’t have to worry about changing patterns routinely during my surgical day. Additionally, the cataract density imaging feature allows me to restrict fragmentation to the nucleus to optimize where the laser energy is used to provide the best fragmentation. I’ve found that feature extremely useful; Streamline lets me reduce the laser energy I’m applying to the eye and avoid issues like sticky cortex that can result in increased phaco time. That makes the cataract density imaging system (Figure 2) a big advantage in terms of both laser energy and time savings.
Avoiding the excimer laser LENSAR with Streamline can also be used on patients with issues related to astigmatism – like those who have refractions that are close to plano from a spherical equivalent standpoint but still have an astigmatism that affects their vision. Now that we have iris registration, there’s definitely a role for Streamline in managing astigmatism correction on a patient – instead of say creating a flap, then using an excimer laser to ablate the cornea to correct for that astigmatism after cataract surgery. So by doing a small or large laser arcuate incisions on the cornea using LENSAR with Streamline, we’re able to reduce the cylinder to the point where uncorrected visual acuity is sufficient to allow refractive cataract patients to see well at distance.
Ulrich-Christoph Welge-Lüβen
Senior Physician and Associate Professor of Glaucoma and Anterior Segment University Clinic Erlangen, Germany I have performed more than 8,000 procedures using manual rhexes and standard phacoemulsification during my career to date. With the introduction to the laser-assisted cataract surgery, I had to adjust my surgical approach to optimize the procedure. For instance, I used a basic setup to perform capsulotomy initially, and I often had difficulty with cortex removal, as the fibers seemed to adhere to the edge of the capsulotomy. I had to take my irrigation/aspiration system under the edge of the capsulorhexis to remove them – something that no surgeon likes to do. But we reduced the laser energy during the capsulotomy we achieved much better results. The cortex fibers did not stick anymore to the edge of the capsulotomy and fibers were free hanging in the center. So cortex removal was greatly improved, by using low energy in capsulotomy, and was as easy as in standard phacoemulsification. Effective diagnosis with 3D Augmented Reality imaging I’ve recently begun using the LENSAR and its 3D Augmented Reality feature. The cataract density imaging and automatic lens fragmentation patterns features that Streamline provides are very impressive (Figure 2). I’ve found that Streamline’s classification system is very reliable and adapts to the individual lens characteristics by determining optimized fragmentation patterns – so I can use the lowest appropriate energy settings, which I feel is always the safest approach. I’ve seen a reduction of phaco energy by around 60 percent! The non-applanating patient interface should also cause less damage to the cornea than traditional applanating methods. The “perfect capsulotomy” That patient interface actually serves an even more important function, namely letting me create what I consider the perfect capsulotomy. When I use the LENSAR with Streamline, I can ensure that the IOL that I implant is perfectly covered by the edges of the anterior capsule. That’s always beneficial, but it’s especially important as about one in five of my patients receive multifocal lenses. In that type of procedure, having the edges of the artificial lens covered by the edges of the capsulotomy is a real must. So far, I’ve performed 115 capsulotomies with the laser and I haven’t had a single problem or complication. I always compare the technology to cars, which is a great analogy to use with patients – a standard phaco is a Volkswagen Golf, but a femtosecond laser like LENSAR with Streamline is a Mercedes S Class. Automation helps beget safety Because I focus so much on safety, I’ve found LENSAR with Streamline’s preoperative assessment tools extremely useful. Streamline has wireless data transfer from the Cassini Corneal Shape Analyzer, which avoids transcription errors; automatic fragmentation planning, including cataract density imaging; the ability to predict and minimize the amount of laser energy that will be needed; and the ability to include arcuate incisions in the surgical plan, which may reduce the need for toric lens implantation, and if I need a toric IOL, steep axis corneal marks that I can use to guide lens placement. All of these things can be done on a single machine during a single procedure, so if something unexpected does arise, the surgeon can deal with it immediately. Safety was the primary factor I considered when I decided to buy a femtosecond laser, but efficiency was also important – in the form of the workflow efficiency offered by automation and wireless transfer. I’ve been very happy with LENSAR with Streamline since I bought it; if I had to make the choice a second time, I’d definitely opt for the LENSAR with Streamline again – especially as the service from Topcon was excellent, both in setting it up and in training me to use it. In fact, if I were to have an IOL implanted myself, I’d like the doctor to treat me with LENSAR with Streamline, because I feel it’s safer for the patient than other devices.The Evolution of Cataract Surgery
1949: Harold Ridley implants first intraocular lens (IOL)1959: Cornelius Binkhorst coins the term “pseudophakia”
1967: Svyatoslav Fyodorov publishes first IOL power formula
1967: Charles Kelman introduces phacoemulsification to cataract surgery
1972: Nicholas Brown pioneers use of Scheimpflug imaging for cataracts
1975: Jack Hartstein patents bifocal IOLs
1990: John Shepherd invents in-the-bag fracturing, hydration and quartering of nucleus for phaco
1998: First toric IOLs to correct astigmatic vision introduced
2001: First use of a femtosecond laser in ophthalmic surgery (LASIK flap creation)
2008: Zoltan Nagy performs the first femtosecond laser-assisted anterior capsulotomy
2010: First femtosecond laser gains FDA approval for cataract surgery
2011: First femtosecond laser gains CE mark for cataract surgery
2015: LENSAR with Streamline launched
