To The New Femtosecond Laser Generation
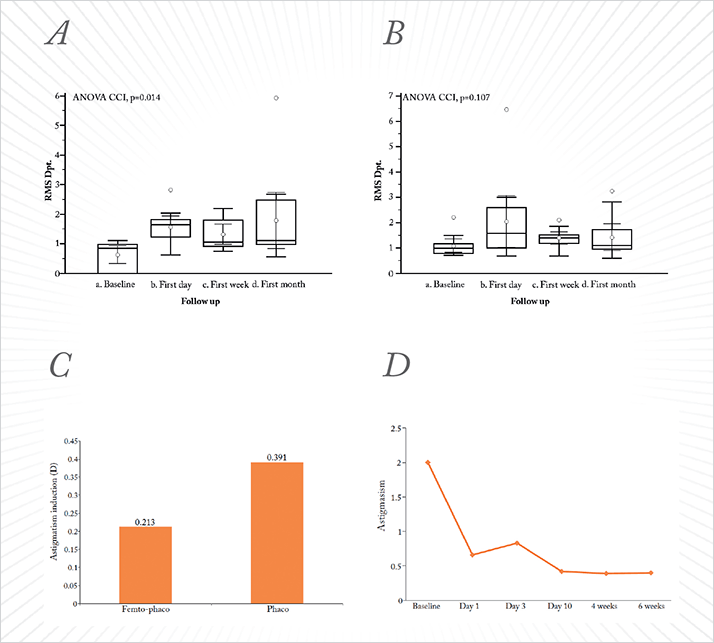
Highlights from Ziemer Ophthalmic Systems AG’s Satellite Symposium, “It’s Time to Make a Move: The New Femtosecond Laser Generation”, held on September 13, 2014 at the XXXIII ESCRS Congress, London, UK. The Ziemer FEMTO LDV Z8 femtosecond laser has been designed specifically as an all-in-one device that can be used for both corneal and cataract procedures. Four eminent ophthalmologists described their real-life experiences with the Z8.Bojan Pajic The right femtosecond laser can be extremely useful to a cataract surgeon. These instruments can perform reproducible and precise capsulotomies and lens fragmentations, create clear corneal incisions (CCIs) for anterior chamber entry, and, when necessary, make arcuate incisions for astigmatism correction. Clear corneal and arcuate incisions with the FEMTO LDV Z6 I am fortunate enough to use a Ziemer FEMTO LDV Z6 PowerPlus femtosecond laser in my clinic, and I wanted to determine whether arcuate and clear corneal incisions (CCIs) made with the FEMTO LDV Z6 produce better clinical outcomes for patients than conventional incisions. I performed a prospective case series that involved 42 eyes (21 patients; 14 males, 7 females; mean age 74.9±6.7 years): one eye received femtosecond laser-assisted incisions with the Z6 whereas conventional incisions were performed on the other. The CCIs can be sculpted for access to the anterior chamber, with one main incision and up to two paracenteses. Highly flexible software allows for topographically matched and fully custom-designed incisions. I assessed patients’ root-mean square (RMS) higher order abberations (HOAs) before surgery and then one day, one week, and one month afterwards (Figure 1A). No significant changes between pre- and post-operative RMS HOAs were observed in the Z6-treated eyes throughout the one month follow-up period (p=0.107). However, eyes that underwent conventional cataract surgery had significantly elevated RMS HOAs (p=0.014) during the same period (Figure 1B). Furthermore, surgically-induced astigmatism was lower in the laser-operated eyes (0.213 D) than in eyes that received conventional cataract surgery (0.391 D; Figure 1C). If we focus on the effect of the Z6’s arcuate incisions (Figure 1D), we see that on average, we started with a baseline astigmatism of 2 D, which was reduced to less than 0.5 D by 10 days post-operatively, and maintained through to the end of the study’s follow-up period at six weeks. Clearly, the patient numbers are relatively small, and larger, multicenter studies are required to validate these data, but I think the fact that the Z6 can perform these precise arcuate incisions to control astigmatism in patients with cataract means that this laser could potentially provide an excellent alternative to multifocal intraocular lenses.
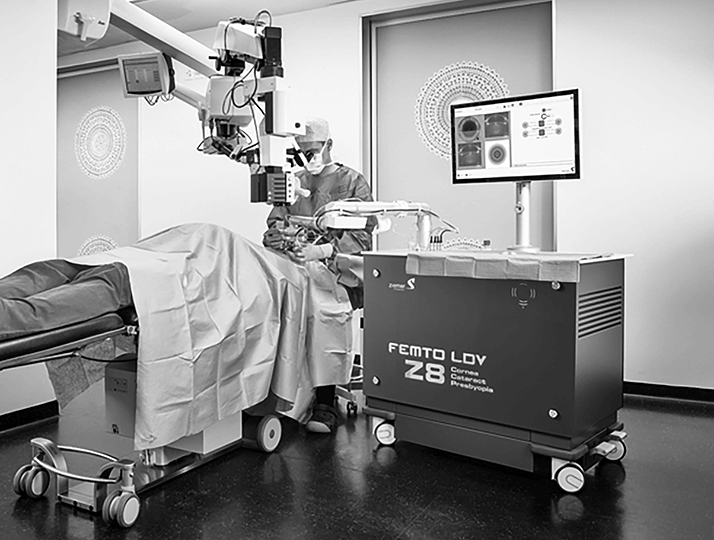
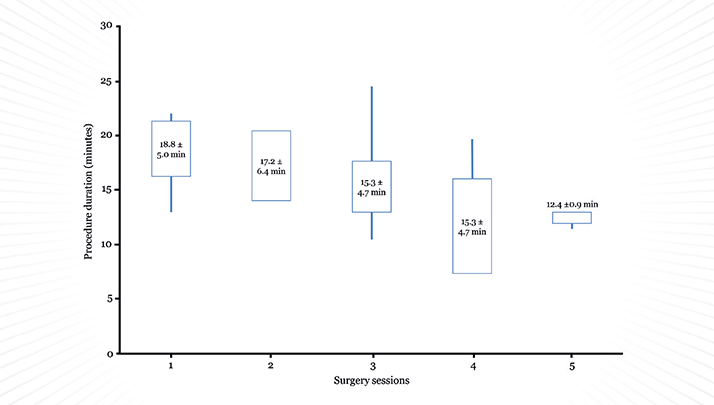
Cataract surgery with the FEMTO LDV Z8 I also have a Ziemer FEMTO LDV Z8, which uses a new liquid patient interface that enables femto-cataract surgery. Anterior capsulotomy, lens fragmentation, as well as LASIK, keratoplasties and more can be performed – all with the same system. I use the Z8 extensively for cataract surgeries in our clinic and I have recently completed a trial where I evaluated its safety and surgical outcomes in patients undergoing capsulotomy and primary lens fragmentation. Of the 117 patients (117 eyes) scheduled to undergo cataract surgery (mean age 72.9±9.3 years; cataract grades 2–4), the Z8 reliably and reproducibly created free-floating capsulotomies, with easily removed discs. The laser performed lens fragmentation well, with excellent resection quality in all patients. Portability improves workflow The Z8 has wheels, which is a far greater advance than you might think. They make the Z8 portable, so rather than having to move the patient under the laser, you can move the laser over the patient, making life easier and saving time during each and every procedure. Because speeding workflow is becoming increasingly important for today’s cataract/refractive surgeon, we decided to assess the time it took to prepare and perform the laser procedures and phacoemulsification. We were able to perform four cataract procedures in an hour after only a few sessions (Table 1; Figure 3 – and the results speak for themselves.
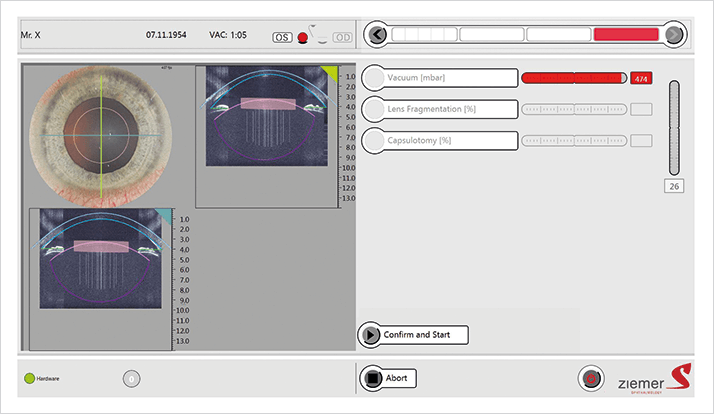
Improving accuracy and speed I have found that the FEMTO LDV Z8 laser’s tissue adaptive pulse management feature – which gives the ability to apply high energy levels to the lens, but lower energy levels to the cornea – results in less gas formation in the lens and fewer intraoperative complications than lasers without these properties. Other features of the Z8 help too, such as its real-time anterior segment imaging, which aids both docking and planning (the XY-axis); the intraoperative optical coherence tomography (OCT) imaging feature (with automatic pupil and limbus recognition) gives me the Z-axis. Together these features allow me to place and visualize the resections and finely adjust their position in all three dimensions (Figure 2). What this means in practice is that the low-pulse energy modules allow reproducible, precise, free-floating capsulotomies. If I specify a 5.0 mm diameter capsulotomy, that’s what I get, every time, and the discs are easy to remove. There’s a fast learning curve with the instrument, and the properties of the femtosecond laser beam and the mobility of the laser unit means that I have a fast workflow too.
Luis Izquierdo Jr.
The Ziemer FEMTO LDV Z8 is the pinnacle of Ziemer’s current range of femtosecond lasers. It’s a versatile device that offers everything the Z6 offers (LASIK, resection for intracorneal rings and intrastromal pockets, lamellar and penetrating keratoplasty, and clear corneal and arcuate incisions) using the applanation interface, but the new liquid interface opens up a new possibility: femto-cataract surgery. This interface allows you to perform anterior capsulotomies and lens fragmentation, as well as offering an additional way of achieving clear corneal and arcuate incisions. This can be particularly useful on occasion; for example, with premium toric or multifocal IOLs. Patients with multifocal lenses can tolerate no more than around 0.5 to 0.75 D of cylinder – and this is something that we can correct during the same femto-cataract surgery procedure, making the Z8 a great platform especially with multifocal lenses. Of course, you can perform very precise intrastromal astigmatic keratotomy with the Z6 and Z8 if you need to correct greater astigmatism in this context.
The intraoperative OCT is also a great feature. It gives you automatic detection of the ocular structures, accurate positioning of any planned beam trajectories, helping you to integrate corneal and cataract surgery, plus it lets the surgeon customize what’s performed to his or her liking.
The docking system is very easy to use, meaning that capsulotomies are easy to perform – even in patients with very small eyes, like we commonly see in Peru. You get a free-floating capsulotomy, and here I’d like to share a pearl. Using forceps is the hard way to remove that capsule; use visco-pressure or aspiration to remove it. Fragmentation in lenses with even hard nuclei is simple and rapid – eight cuts to the lens can be made in a matter of a few seconds, and phacoemulsification is easily performed.
In summary, I find the Z8 easy to integrate into my workflow, as it’s flexible and fast and as it has both the liquid and applanation interfaces and intraoperative OCT, it means that I can plan and perform a whole suite of corneal, cataract and
refractive procedures using the same laser.
Jod Mehta George Orwell once wrote, “All animals are equal, but some are more equal than others.” This statement could equally apply to femtosecond lasers. The term “femtosecond laser” is used to describe products from any number of different manufacturers, and it implies that all of these instruments are the same – but that’s completely untrue. Energy and power are not interchangeable terms Although energy and power are linked when discussing femtosecond lasers, they are not interchangeable terms: power = energy × time. Even extremely powerful lasers can impart relatively low energy into tissue if you have a very fast, high-repetition laser. Beam movement speed varies by manufacturer, as do the patterns used to form the resection plane (Ziemer lasers use a raster pattern, whereas others use an Archimedean spiral). Resection plane differences are caused by two things – spot separation and line separation – and when you evaluate the literature, I recommend that you note the authors’ recorded spot and line separation settings before trying to replicate results in your own clinic. Are all femtosecond lasers equal? Do different femtosecond lasers have different effects on corneal tissue? I wanted to find out. Using a helium ion microscope, my colleagues and I compared the effects of a microjoule femtosecond laser system with a low energy, nanojoule system, by making corneal flaps of 110 µm thickness and 7.9 mm diameter in cadaver human corneas (1). We found that the higher-energy laser system produces a crater shape on the corneal surface, whereas the low-energy system created an annular ring – giving rise to a more precise incision and inflicting less in the way of collateral damage. The Ziemer laser has very high focusing power, meaning you can get much tighter Z-axis focusing even with low pulse energy, compared with higher pulse energy systems.
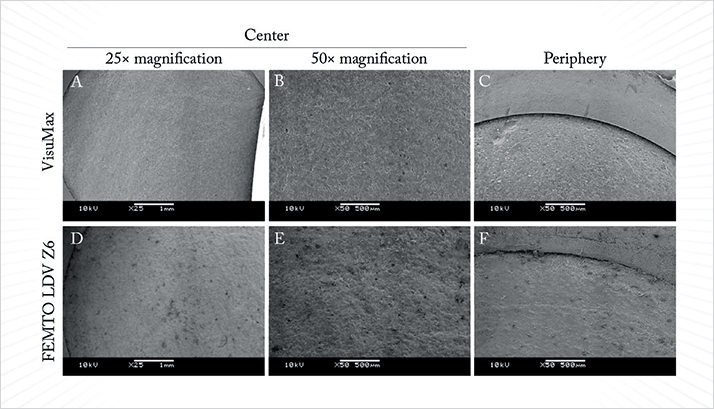
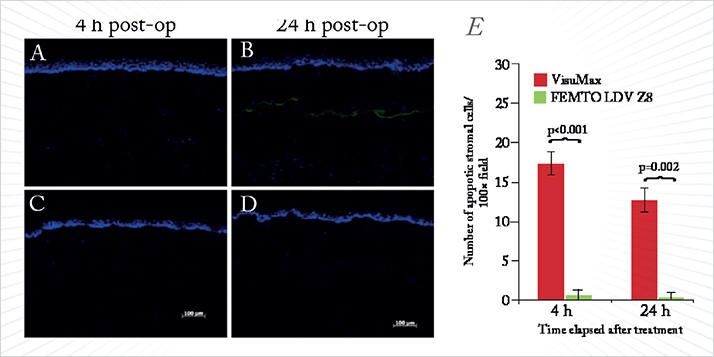
Studies using a rabbit experimental model for LASIK are one thing – but can we demonstrate a difference between these femtosecond laser systems in human corneal tissue? We created corneal flaps (110 µm thickness, 8.2 mm diameter) in human cadaveric corneas, lifted and directly repositioned the flaps, then immediately processed the corneas for scanning electron microscopy – the sections are shown in Figure 1 (2). If we look at high magnification, the Ziemer laser’s flaps (Figure 1D,E) are as equally smooth as those created by the VisuMax laser (Figure 1A,B). However, we saw distinct wound healing advantages and immune responses using the lower-energy nanojoule femtosecond laser; it did not cause significant cell damage or keratocyte injury (Figure 2), or elicit a measurable healing response – meaning that lower-energy femtosecond lasers have the potential to reduce scar formation in stromal surgery. One of the potential issues with low-energy systems is that although you might get reduced flap adhesion, as there’s less wound healing. We assessed the flap strength from both systems and there were no significant differences between them. If you remember back to the first publications on high-energy femtosecond lasers, there was a whole cacophony of side effects: transient light sensitivity, collateral tissue damage, and vertical gas breakthrough. The Z8 – like the Z6 before it – provides a low-energy femtosecond laser that provides a high-speed pattern repetition. You get the benefits of low energy without sacrificing laser cutting speed. You get a precise core diameter, a better shape of your laser pulse on the corneal tissue itself, and you require less Z-axis focusing: in essence, you get a more precisely defined incision compared with higher-energy femtosecond lasers. You can only get these benefits with a nanojoule-power femtosecond laser (1).
References
- AK Riau, et al., “Nanoscale analysis of human corneal collagen lamellae following femtosecond laser dissection using helium ion microscopy”, J Biomed Nanotech., 10, 1552–1562 (2014). PMID: 25016655.
- AK Riau, et al., “Comparative study of nJ- and μJ-energy level femtosecond lasers: evaluation of flap adhesion strength, stromal bed quality, and tissue responses”, Invest Ophthalmol Vis Sci., 55, 3186–94 (2014). PMID: 24764066.
Theo Seiler Using the FEMTO LDV Z8 during femtosecond laser-assisted cataract surgery is both simple and fast – you can go from bringing the laser to the patient, to completing a capsulotomy in two minutes, ready to pre-chop the lens ahead of phacoemulsification. The fact that it is mobile means not only that you don’t have to move patients to the laser, you bring the laser to them – helping speed workflow in busy cataract/refractive practices – but you can also easily move the laser to another room or even a practice nearby, as it is easily loaded into a van. You can share the costs of the femtosecond laser with another clinic – on Monday, Tuesday and Wednesday, clinic A does surgery with the Z8, and on Thursday and Friday, clinic B is using it. Why not? It’s a distinct advantage over larger, immovable machines…

What we have learned from Jod Mehta is that if we have low pulse energy, we get minimal cavitation gas. This is important for two key reasons: we can perform keratoplasty with minimal damage to the cornea, and it removes the potential for high pressure-induced capsule rupture. It also lets the surgeon perform lens fragmentation before the capsulotomy, meaning that incisions can be made with greater precision, as there is no air between the laser and the site of fragmentation. Changing the patient interface can transform the Z8 into a Z6, which opens up the possibility of performing LASIK surgery with the same laser – and because the Z8 is portable – in a different room. As I am principally a corneal surgeon, it also means that I can perform keratoplasties like UT-DSEK, top-hat PKP and DALK with the same instrument. To sum up, I would say that the FEMTO LDV Z8 offers mobility, powerful optics and high repetition rates, all with a low energy femtosecond laser. You get minimal cavitation gas development with it and you can perform keratoplasty with minimal changes to the cornea. Like the Z8 itself, perhaps it’s time to move over to the new generation of femtosecond lasers.
