
Most glaucoma filtration surgeries involve creating a new uncontrolled drainage channel for the aqueous humor outflow, which requires full penetration of the sclera (e.g. trabeculectomy, GDD); the outcome of that radical procedure is trauma to the eye’s natural circulation process of the aqueous humor, leading to many post-surgical complications, adverse events and side effects.
Increasing aqueous humor outflow in an effective manner shouldn’t require a radical solution that is not part of the eye’s natural process – it can be performed in a safe manner, by simply reducing the resistance of the eye’s natural filtration process. A CO2 laser-assisted sclerectomy surgery (CLASS), from IOPtima, is designed to do just that. This novel approach uses infrared CO2 laser technology to gently remove microscopic layers of tissue from precisely targeted regions of the sclera. And because the infrared laser cannot penetrate wet tissues, the system has the benefit of an intrinsic safety feature.
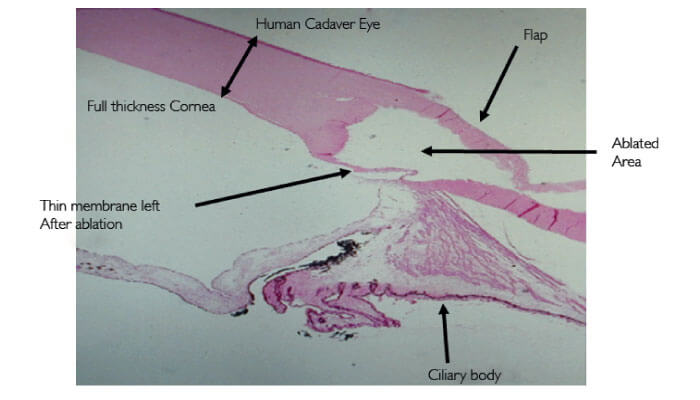
How does it work? In brief, the IOPtiMate device (Figure 1) generates controlled ablations above the Schlemm’s canal region. This operation thins the scleral wall layer by layer in a highly controlled manner until eventually removing Schlemm’s canal, but safely leaving a thin tissue layer intact – non-penetrating into the anterior chamber (Figures 2, 3). The remaining intact thin layer is permeable to intraocular aqueous humor – which can now follow a pressure gradient and leave the eye – but, importantly, it does not change the natural filtration pathway – it includes the removal of the major resistance to aqueous outflow. Keeping the natural drainage system of the eye intact, rather than relying on the construction of new, non-physiological channels, enables a much better safety profile with marginally less post-operative complications, together with similar efficacy. And most importantly, the key characteristic of the CO2 laser is that it’s highly absorbed by fluid, which generates a self-regulated safety mechanism to the procedure. Once we reached to the desired depth with the laser ablations, enabling aqueous outflow, the laser’s operation are no longer effective on the percolated area. All of this makes the laser-based technology to be a safe, accurate and reproducible technique that is greatly simplifying the manual deep sclerectomy procedures.
The expected advantages of CLASS are clear: as a procedure that is both non-penetrating and does not require implantation of foreign bodies, it would be expected to have fewer safety concerns than other glaucoma filtration surgeries. But how does CLASS fare in practice? Top marks, so far: five-year study outcomes (1) indicate IOP reductions of over 40 percent. Furthermore, post-operative complications are significantly lower in number and are transient.
In a recent comparative study (2) published in September 2018 of phacoemulsification combined with CO2 laser-assisted sclerotomy vs. phacoemulsification combined with trabeculectomy in patients with open-angle glaucoma, led by Juan Carlos Izquierdo Villavicencio (MD and Chief of Glaucoma, Department of Ophthalmology, Oftalmosalud Eye Institute, Lima, Peru), CLASS showed similar efficacy to trabeculectomy patients in terms of IOP and medication reduction, but the CLASS-treated patients enjoyed better visual acuity outcomes, with lower rates of post-operative complications than the conventional trabeculectomy method. As Izquierdo states: “Glaucoma is one of the leading causes of vision loss and blindness globally. It is critical that we continue to explore the best surgical procedures possible – those that are safe, accurate, and provide optimal
postoperative results.
“The outcomes of this comparative study have been crucially important in helping us to identify and maintain adequate control of intraocular pressure with the introduction of the IOPtiMate system. The results of the CLASS group have clearly shown the safety and efficacy of CLASS as a viable and successful alternative surgical procedure to traditional trabeculectomy.”
To summarize, CLASS procedure has been proven with long-term efficacy in terms of lowering IOP and medication reduction, and as a safe procedure with low number and transient post-operative complications.
Notwithstanding these positive outcomes in combined cataract-glaucoma surgery, CLASS is currently indicated for patients with mild, moderate or severe primary or secondary Open-Angle Glaucoma (OAG), including Pseudo-Exfoliative Glaucoma (PEXG). CLASS has also been proven with long-term efficacy in terms of lowering IOP and medication reduction, and as a safe procedure with low-number and transient postoperative complications. Its developer, IOPtima, is making the system broadly available through a flexible business model that can accommodate both private and public hospitals, and welcomes enquiries from interested parties.

References
- Five Year Follow Up of CO2 Laser Assisted Sclerectomy Surgery (CLASS) - http://ioptima.co.il/wp content/uploads/2016/06/poster-10.06.2016-14.57.pdf JCI Villavicencio et al., “Comparative clinical results of phacoemulsification combined with CO2 laser-assisted sclerotomy vs. phacoemulsification combined with trabeculectomy in patients with open-angle glaucoma”, J Clin Exp Ophthalmol, 9, 5 (2018). DOI: 10.4172/2155-9570.1000749.
