- There’s a long list of reasons why hypermature, rock-hard cataracts are challenging cases
- Eyes with such advanced cataracts often have a number of ocular comorbidities that you need to be aware of
- Having a surgical strategy in place is essential to minimize the risks associated with this procedure, and to ensure the patient experiences a successful surgery
- I share my ten top insights into dealing with such cases
Performing cataract surgery in patients with extremely dense, rock-hard cataracts can be a considerable challenge for even the most experienced cataract surgeon. These highly dense – and therefore highly opaque – cataracts makes preoperative assessment difficult, and perioperative visualization of the capsule even harder. These lenses are hard – and therefore hard to maneuver, and this is compounded by the fact that such lenses typically occupy a larger volume than lenses with less advanced cataract – meaning that the surgeon has even less space to work in than usual. Further, as cataracts develop, the lens capsule thins and becomes ever more fragile, zonules weaken, so by the time you have a “Hard Rock” cataract, you almost always have a particularly challenging case to deal with. This type of cataract requires longer phaco times, higher energy levels, and carries a higher subsequent risk of corneal decompensation. Sun Tzu wrote in The Art of War: “Know your enemy and know yourself and you can fight a hundred battles without disaster.” I would apply the same thinking to this type of surgery: first understand what you’re dealing with, then plan to conquer accordingly.
With that in mind, I have some tips for dealing with these difficult cases (see “Top 10 Tips for Success”). Cases of “Hard Rock” cataracts are clearly a challenge – and it’s not just down to the density of the cataract (although that clearly plays a part). There’s a minefield of comorbidities and potential issues to navigate through, but if you’re prepared, have the right tools, and a strategy to deal with the issues, then you can deal with them calmly, effectively and without drama – which is exactly what you want when performing surgery.
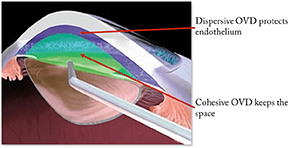
1. Use OVD to protect the endothelium
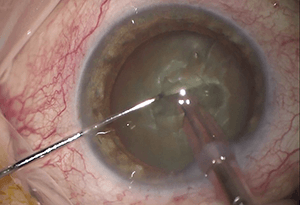
As the phacoemulsification required to deal with the hypermature cataract is likely to take longer – and require greater energy levels – than your typical procedure, it is prudent to use OVD to protect the endothelium. I recommend using the soft-shell technique – first placing the dispersive OVD to coat the corneal endothelium, then the cohesive OVD injected centrally to flatten the anterior chamber lens capsule, deepening the anterior chamber, and forcing the dispersive OVD to move towards the cornea.
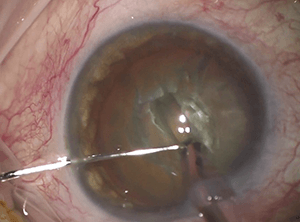
2. Embrace vital dyes
Vital dyes like trypan blue can be extremely useful in cases of rock-hard cataracts; it can be used to stain the anterior capsule, making it easier to visualize during a manual capsulorhexis, and it has shown to decrease its elasticity, which further helps the maneuverability of the capsule during the rhexis procedure, especially in cases of associated zonular weakness. Further, I would recommend placing the trypan blue under the OVD as opposed to under air, as this helps avoid sudden potential changes in anterior chamber depth and intraocular pressure, and should help preserve the lens zonular status – I would suggest that using air (rather than OVD) in this situation increases the risk of vitreous prolapse, and, since trypan blue has proven to be endothelium friendly, this has become an unnecessary surgical step.
3. Make a bigger ‘rhexis than usual
A larger-diameter capsulorhexis (around 5.5. mm, bigger than the usual 5.0 mm) helps avoid segments hooking each other, and it makes it easier to perform segment emulsification.
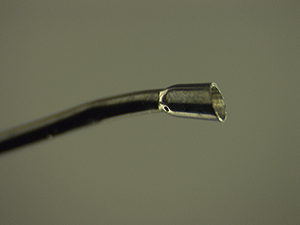
4. If you can, use a 1.1 mm Kelman 30–45° flared ABS tip
You might thank me later on this one. The Kelman flared tip gives a larger area of phacoemulsification and good holdability. The small (ABS) hole in the middle of the tip should mean that a steady flow rate is maintained during occlusion, while simultaneously decreasing the chance of a surge effect when the tip is occluded.
5. If you’re using an OZil phaco tip, don’t use IP to keep the phaco tip free
This one that applies to my own setup – Alcon’s Infiniti – but if you’re using the OZil Intelligent Phaco (IP) tip, don’t use IP to keep the tip free. I find that during phacoemulsification, I need to use some longitudinal ultrasound – around 25 to 30 percent – to ensure a smooth phaco procedure. Further, short pulses of longitudinal energy (like IP) are not enough to mobilize small nuclear fragments inside the phaco tip, and this just makes the process inefficient.
6. Make a big central groove
Remember, you’re dealing with a bigger lens than usual, so making a big central groove when you’re dividing and conquering will give you more space for future maneuvers.
7. Keep applying that OVD!
A large nucleus tends to hold back the posterior capsule. However, the risk of injuring the posterior capsule with the phaco tip increases with the amount of nucleus removed. Once you’ve removed most of the nucleus, use a little dispersive OVD to inflate the posterior chamber and push back the posterior capsule – and protect against injury from the phaco tip.
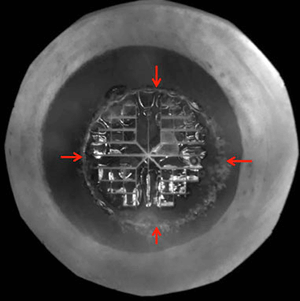
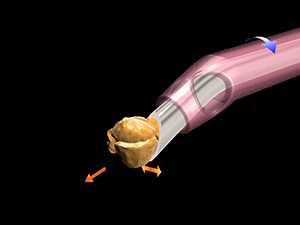
8. Impale the nucleus before cracking – it is safer!
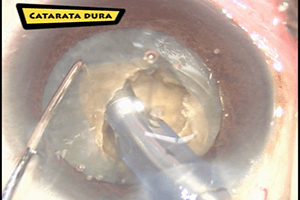
Instead of just doing our traditional stop & chop technique, in which the nucleus is cracked by just applying pressure against both walls of the groove without really holding the nucleus itself, a useful tip for dealing with hard lenses is to rotate your nucleus, positioning your groove horizontally (as shown above), impale your phaco tip into the distal wall of the groove which will secure holdability, and then use your second instrument against the proximal wall off the groove to create the crack (as shown below). This maneuver provides more control, which is especially helpful in this setting, since in harder lenses, breaking the fibers of the posterior shield can be very challenging without proper countertraction.
After the chop has been completed, just resume your standard phaco technique for quadrant removal.
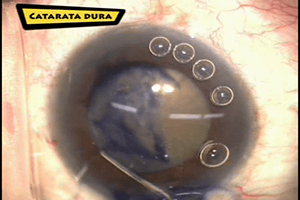
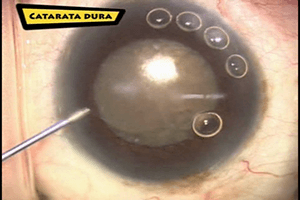
9. Stop and chop
Break the nucleus up into more segments than usual – six to eight – to make the phacoemulsification of each part a bit more manageable.
10. Consider using a capsular tension ring
Capsular tension rings (CTRs) provide support during the cataract extraction procedure, and can help ensure long-term IOL stabilization. As there is always some concern about zonular stability in patients with rock-hard cataracts, CTRs act to stabilize the entire zonular apparatus, by recruiting tension from existing zonules, and redistributing the forces to the remaining weaker zonules. They also help prevent postoperative capsular phimosis – something that, again, is more common in patients with hard cataracts.