Can vision loss caused by damage to the optic nerve ever be restored? Bernhard Sabel and his team seem to think so, and over the past few years they have been attempting to use repetitive transorbital alternating current stimulation (rtACS) to partially restore vision in patients with optic nerve damage. The noninvasive procedure involves applying biphasic pulses of electrical current (8–25 Hz) through electrodes placed on the skin around the orbital cavity. “This field is popular, but not without controversy,” notes Sabel.
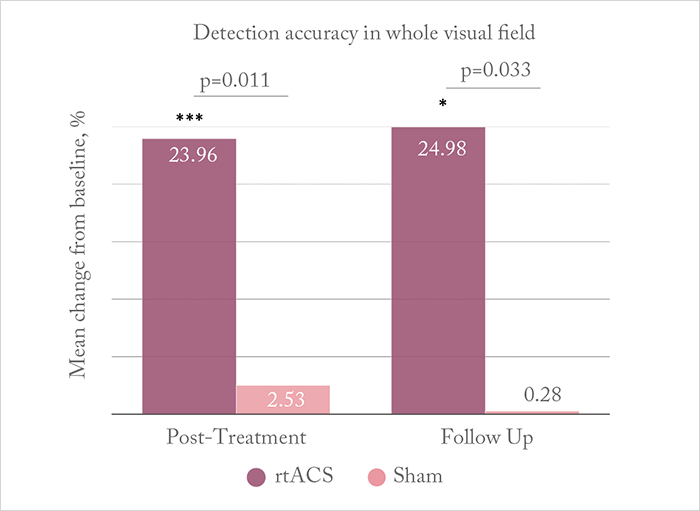
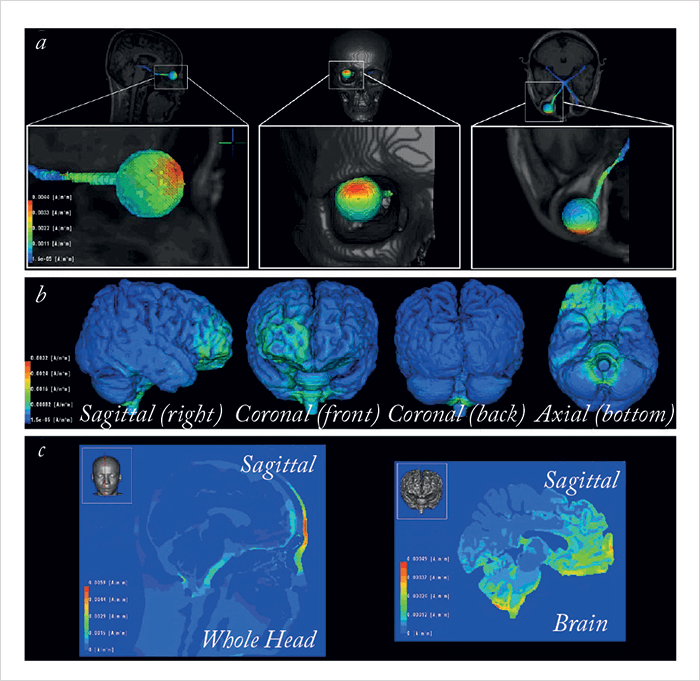
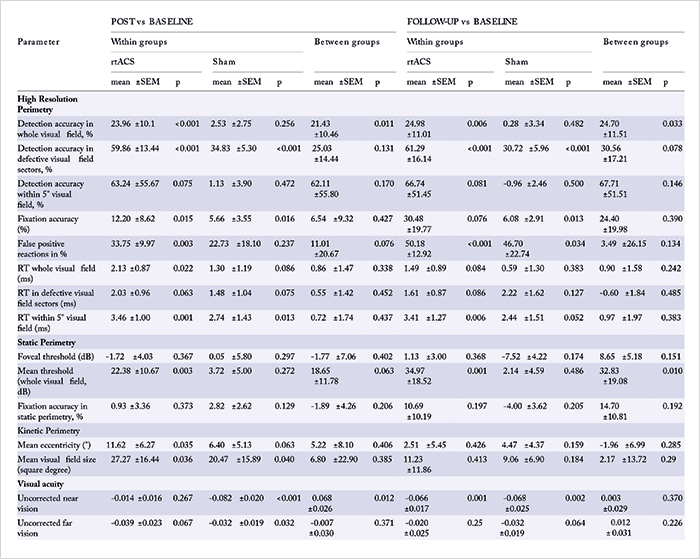
Could it work? He proposes that rtACS modulates brain plasticity and re-synchronizes functional neural networks disrupted when vision is lost. According to Sabel, “Administering current stimulation through the eye causes retinal ganglion cells to fire intensely”, although “the precise mechanism of action is unknown”. Nevertheless, the team – and others – have shown visual field improvements with rtACS in early studies performed in small patient groups (1)(2)(3)(4). Now, they have published results from, what Sabel believes to be, the first large-sample, multicenter trial that shows efficacy (5). In their prospective, double-blind, sham-controlled trial, patients with optic neuropathy and residual vision (of various causalities) were randomized to receive 10 treatments of rtACS (n=45) or sham stimulation (n=37) over two “weekday courses” (Monday–Friday). The team assessed 15 different visual parameters (through high-resolution, static and kinetic perimetry, and visual acuity assessments) at baseline, after 10 treatments, and after two months of follow-up. What they found was, at 10 days following rtACS stimulation, whole visual field detection accuracy was significantly improved compared with baseline levels and the sham-treatment group; at follow-up, these improvements were maintained (Figure 1). For all results, see Table 1. The team also modelled rtACS current flow using computer simulation models (Figure 2), suggesting that “the stimulation current propagates through the eyeball and optic nerve to subcortical and midbrain regions, with secondary stimulation in both the brainstem and in cerebellar regions” (5).
No patient reported discomfort during stimulation, but there were reports of transient vertigo by two rtACS patients in a total of five sessions, and mild headache (one incidence from one patient in each study group). After stimulation, six patients (four rtACS; two sham) reported mild headaches and 20 patients reported cutaneous sensations (12 rtACS; eight sham). One sham patient reported persistent vertigo for 30 minutes after each session.
Sabel concedes that additional studies are needed, but believes that his group’s results “warrant the use of rtACS treatment in a clinical setting to activate residual vision by brain network re-synchronization” as it can “partially restore vision in patients with stable vision loss caused by optic nerve damage.” Describing the team’s next steps, Sabel says they will work on “optimizing the stimulation protocol and finding new ways to improve the efficacy of the therapy.” Perhaps most pertinently, and crucially for wider acceptance, he adds, “We also need to learn more about the mechanism of action.”
References
- M Bola et al., “Brain functional connectivity network breakdown and restoration in blindness”, Neurology, 83, 542–551 (2014). PMID: 24991030. BA Sabel et al., “Non-invasive alternating current stimulation improves vision in optic neuropathy”, Restor Neurol Neurosci, 29, 493–505 (2011). PMID: 22124039. C Gall et al., “Noninvasive transorbital alternating current stimulation improved subjective visual field functioning and vision-related quality of life in optic neuropathy”, Brain Stimul, 4, 175–188 (2011). PMID: 21981853. S Schmidt et al., “Progressive enhancement of alpha activity and visual function in patients with optic neuropathy: a two-week repeated session alternating current stimulation study”, Brain Stimul, 6, 87–93 (2013). PMID: 22537864. C Gall et al., “Alternating current stimulation for vision restoration after optic nerve damage: a randomized clinical trial”, PLoS One, 11, e0156134 (2016). PMID: 27355577.
