Current trends in refractive surgery point to the use of implantable contact lens (ICL) rising steadily above all others. I believe the option of “additive” technology, using a small incision along with reliable visual outcomes, makes the procedure highly attractive for those seeking vision correction procedures.
ICLs and their role today
For many moderately to highly myopic patients who want to be spectacle-free, ICLs may well be the only safe option; corneal refractive surgery and refractive lens exchange are the alternatives, but they both carry risks and disadvantages. Corneal refractive surgery is not always possible for high refractive errors because it involves removal of corneal tissue beyond the safety limit to achieve full correction. Refractive lens exchange or lens replacement carries a higher risk of retinal detachment in younger myopic eyes, especially in males and eyes with axial lengths of greater than 25.00 mm. The presence of any peripheral retinal pathology, such as lattice retinal degeneration, is also a risk factor. Additionally, in younger patients, the loss of the crystalline lens results in a complete loss of accommodation, and therefore, the need for a multifocal lens to provide some near vision. However, this can result in an unsatisfactory visual quality and, in the case of a monofocal or extended depth of focus lens, loss of near vision.
As an additive option with low adverse incidents, ICLs are a good and safe refractive option for patients.
Key preoperative considerations
The ICL is a viable option for patients between the ages of 21 and 60 with a stable refraction (less than 0.5 D change for one year) and a clear crystalline lens. Anterior chamber depth (ACD) must be ≥ 2.8 mm, as measured from the corneal endothelium to the anterior lens capsule to avoid angle compromise. ACD is best evaluated by either Scheimpflug, ultrasound biomicroscopy, or anterior segment OCT (1).
Ideally, patients must also meet minimum endothelial cell count (ECC) criteria and have no ocular pathology, such as compromised corneal endothelium, iritis, iris atrophy, rubeosis iridis, cataract, glaucoma, or retinal disorders (2).
Eight-point guide for a simpler surgical procedure
- Good pupil dilation is vital to facilitate implantation.
- The lens will be implanted through a 3-mm clear cornea or limbal, self-sealing incision, usually under topical anesthesia.
- After the incision is made, the anterior chamber is filled with a viscoelastic device, preferably Ocucoat (Bausch + Lomb, Bridgewater, NJ).
- To load and position the ICL, I use the Daya ICL Forceps (MicroSurgical Technology, Redmond, WA) – see “The Need for New Forceps.” This ICL loading system with a central opening enables good visualization of the ICL as it is grasped, ensuring centration between the footplates with little danger of rotation when being pulled through the cartridge. Rotation can lead to the lens unfolding upside down in the anterior chamber. The high-quality undulation within the graspers (see Figure 1) provides a secure hold of the ICL without risk of damage.
- Following lens loading, the ICL (see “ICL Choice”) is slowly injected into the AC and correct unfolding is assisted where required by a second instrument, such as a Lester pusher or cannula. The lens is then rotated to its correct orientation and the footplates are very gently positioned under the iris.
- The OVD is then removed by irrigation and aspiration, and wounds are checked to ensure there is no leak. Intracameral antibiotics are instilled, and if both eyes are being operated sequentially, Cefuroxime is used in one eye and Moxifloxacin in the other.
- Post operatively, patients are prescribed topical antibiotics for a week and corticosteroids tapering over a four-week period.
- Visual recovery is quick, with most patients seeing very well within one- or two-days post-procedure and complete recovery occurring at about two weeks later.
Figures 1a and 1b. Daya ICL Forceps featuring undulated graspers with rounded edges, viewing window, and a clear distinction of the blue anterior portion of the forceps. Figures courtesy of Sheraz Daya.
The Need for New Forceps
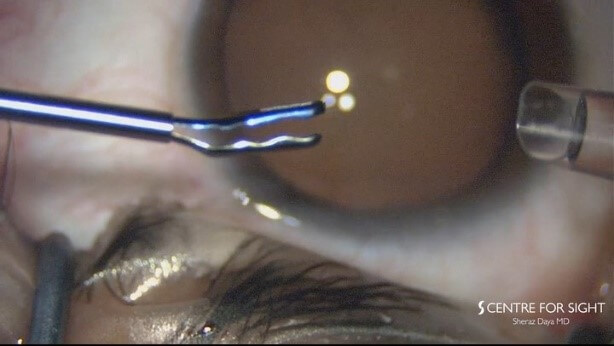
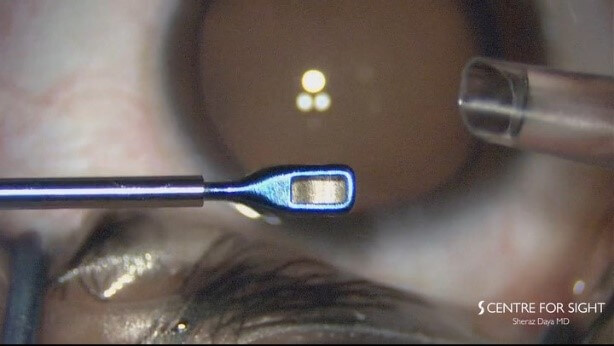
With traditional forceps design, I was unable see how much of the lens I was holding or where it was being grasped. With the new MST Daya ICL Forceps, the viewing window (see Figure 1) allows maximum visibility of the optic during loading, thereby avoiding inaccurate positioning of the lens (see Figure 2), while clear distinction of the blue anterior portion of the forceps (also Figure 1) enhances optic visualization, ensuring correct ICL orientation.
I previously found that when I grasped the lens, the top of the instrument had sharp edges that would scratch against the cartridge, taking off pieces of plastic and creating tiny loose plastic fragments. To solve that problem, we developed rounded edges (again, see Figure 1) on the tip and front of the forceps, ensuring gentle – and, crucially, non-abrasive – contact with the lens and injection cartridge.

ICL Choice
With the novel V4C new generation myopic ICL, the midpoint of the lens has a small opening that allows equalization of pressure between the anterior and posterior chambers thus eliminating the risk of pupil block – and avoiding the need for peripheral iridotomies are avoided with this new ICL.
Conclusion
When I consider the current state of play in refractive surgery, the use of implantable contact lenses and the demand for customised vision are clear trends. Though LASIK remains a popular choice for many patients, ICL is rapidly gaining ground as an alternative – and, for many, a more attractive – option.
Looking far ahead to 2050, when half of the world’s population are expected to be short-sighted (3), it is reassuring to see a great deal of effort being made in myopia control to try and reduce disease severity, which can be blinding. Meanwhile, options for reliable correction of vision will evolve. For the time being, due to the additive – and, in turn, reversible – nature of ICLs, refractive surgeons – and their patients – have an increasingly attractive option.
Financial disclosure: Sheraz Daya has no financial interest in the products discussed; however, the Centre for Sight has received an unrestricted grant from Staar Surgical in the past.
References
- EVO Visian ICL, “Questions” (2021). Available at: https://bit.ly/3aU6AUj
- P Fechner et al., “Correction of myopia by implantation of a concave Worst-iris claw lens into phakic eyes”, J Refract Corneal Surg, 7, 286 (1991). PMID: 1911510
- The Independent, “Short-sightedness increases with every year in education” (2018). Available at: https://bit.ly/3bI7cLX
