
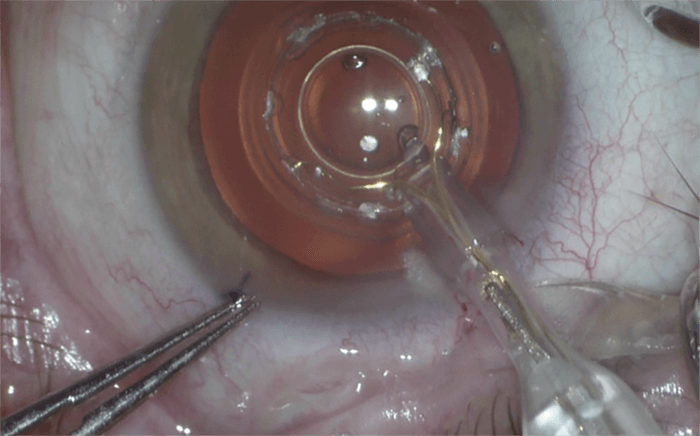
What is Zepto Precision Pulse Capsulotomy? It’s the combination of a power console, fluid isolator, a disposable handpiece with (the genius part): the Zepto tip, which creates circular capsulotomies that are, on average, 2–3 times stronger than those created by CCC or femtosecond lasers (1) – and, at the same time, allows surgeons to easily center the capsulotomy on the visual axis. The Zepto tip (Figure 1) consists of a circular, collapsible micro-molded silicone suction cup that is 6.1 mm in diameter, 1.18 mm in height and contains a 4.4 mm nitinol ring that produces, on average, a 5.2 mm capsulotomy. The ring is inserted using the handpiece through a 2.2 mm or greater clear corneal incision. The Zepto push rod is retracted and the device unfolds back into a circular shape. The surgeon centers the clear suction cup tip over the visual axis, applies suction (gently, but securely locking the tip in place) before a 4 ms pulse of electrical energy is delivered to the nitinol ring. This triggers a rapid phase transition of the water molecules that are trapped between the device and the capsular membrane – instantaneously creating a cleavage plane in the capsular membrane, making a strong capsulotomy, yet remaining gentle on the eye.
My Journey to Zepto
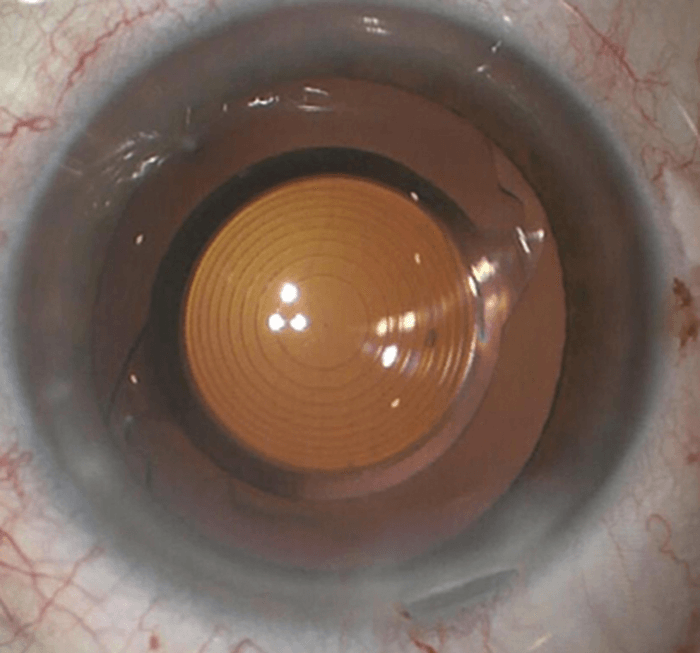
My involvement with the Zepto capsulotomy procedure evolved out of learning the importance of centering cataract surgery on the visual axis. I used to center my manual capsulotomies on the pupil – but I was seeing a lot of patients where I did not get a 360° overlap of the optic; with capsule fibrosis and contraction, I had a higher incidence of lens tilt and decentration than I’d like. When I started using femtosecond lasers, I could consistently achieve a round capsulotomy of the desired size, but I still had inconsistent anterior capsular overlap of the optic. I moved to an OCT-guided femtosecond laser, which helped guide the capsulotomy to the center of the lens. My anterior capsular overlap rate improved – but there was still a significant number of cases where I did not achieve overlap. Why? Patients cannot fixate with a femtosecond laser when it applies suction to the eye. The landmark Chang-Waring paper (2) not only taught me why centering the capsulotomy on the pupil did not give me consistent overlap, but also the Purkinje method of centering on the visual axis, and the importance of patient fixation on the microscope light during the capsulotomy procedure. I went back to manual capsulotomies, marking the cornea with an optical zone marker centered on the visual axis. My anterior capsular overlap rate improved, but I was back to less round and consistently sized capsulotomies. Nevertheless, it is a major challenge following a corneal mark and moving the eye along with the patient’s intermittent fixation and eye movement. I knew that if I could consistently center this important part of cataract surgery on the visual axis, I could further improve my rate of capsular overlap. I then had to opportunity to be a Zepto investigator in their FDA-monitored trial and have adopted this technology into my practice. What has amazed me about the Zepto technology is that I now have a guidance system of a perfectly round device of the proper size that, with the patient fixating on my microscope light, I can center in one motion to guide and create my consistently centered capsulotomy. My rate of anterior capsular overlap of the optic went up tremendously (Figure 2), and Zepto is now a mainstay in my practice. When the capsule contracts over time, tilting or decentration of the optic are minimized because of this consistent overlap – which in turn lessens the chance of the induction of dysphotopsias associated with these processes. I am very happy with Zepto. Vance Thompson, MDReferences
- VM Thompson et al., “Comparison of manual, femtosecond laser and precision pulse capsulotomy edge tear strength in paired human cadaver eyes”, Ophthalmology, 123, 265–274 (2-16). PMID: 26707416. DH Chang, GO Waring, “The subject-fixated coaxially sighted corneal light reflex: a clinical marker for centration of refractive treatments and devices”, Am J Ophthalmol, 158, 863–874 (2014). PMID: 25127696.
