Dr Arthur Cummings is a world-renowned refractive surgeon with extensive experience with Implantable Collamer Lenses (ICLs). He started using STAAR Surgical ICLs over 25 years ago, after encountering eyes that simply weren’t suitable for LASIK or corneal surgery, because of thin corneas, high refractive errors, and eyes with existing dry eye concerns or dry eye risk factors. As the ICL evolved into the EVO ICL, with central Aquaport, and his own experience grew, Dr Cummings’ patient selection criteria for ICL expanded significantly to include ever lower refractive errors, eyes with existing dry eye concerns or dry eye risk factors, suspicious corneas and patients with a preference for a non-laser based, removable (by a surgeon) option.
EVO ICL is now an “equal contender” to the other refractive procedures Dr Cummings offers, so long as there is adequate anterior chamber depth (ACD ≥2.8mm). After all, risk factors for dry eye (1,2) (or Surgically Induced Ocular Surface Discomfort Syndrome/STODS), and other issues that can be exacerbated by a corneal procedure, can be avoided by using the EVO ICL; particularly with higher refractive errors and suspicious corneas, such as ectasia (3) and night vision issues (4,5). This serves to expand the patient pool and increase the refractive range to include lower degrees of myopia; with Dr Cummings explaining how he’s recently treated a -3D myope, who, as an optometrist, elected for EVO ICL over other, corneal based refractive options, after doing thorough research.
As Dr Cummings points out, an experienced ophthalmic surgeon should be able to adapt to using the EVO ICL quickly. Quoting his old mentor, Dr Michiel Kritzinger, Dr Cummings calls it a “butterfly procedure” – requiring both precision and delicacy, which is helped by the EVO ICL’s malleable and forgiving Collamer material. The key points of learning are around patient selection, managing patient expectations, and taking careful measurements to aid in accurate lens selection, to ensure the best possible fit.
Given the short learning curve and additional treatment options that the EVO ICL offers, it’s not surprising that the EVO ICL has become a key part of Dr Cummings’ own refractive offering. Dr Cummings points out that international colleagues have also strongly welcomed the EVO ICL into their practices, to become their predominant procedure for those seeking freedom from the hassles of glasses and contact lenses. Dr Erik Mertens, an ophthalmologist in Antwerp, uses the EVO ICL in two thirds of all his refractive cases, as it achieves excellent visual outcomes (4, 5, 6), doesn’t cause dry eye syndrome (1, 2) (or STODS), and results in the majority of patients seeing 20:20, or better, the very next day. Another colleague, Dr Greg Parkhurst from Texas, offers the EVO ICL to all suitable patients, showing them that there are alternative options available, beyond the more traditional and well-known LASIK option.
Another advantage of the EVO ICL, as a posterior chamber phakic IOL, is that endothelial cell count (ECC) seems unaffected (6) – Dr Cummings reports that neither he, Dr Mertens, nor Dr Parkhurst have seen any issue around ECC* relating to EVO ICL. Careful monitoring is, of course, an essential part of pre- and post-surgical care.
*Please note that endothelial cell loss is listed as a possible complication/adverse reaction in the EVO ICL product Directions For Use (DFU).
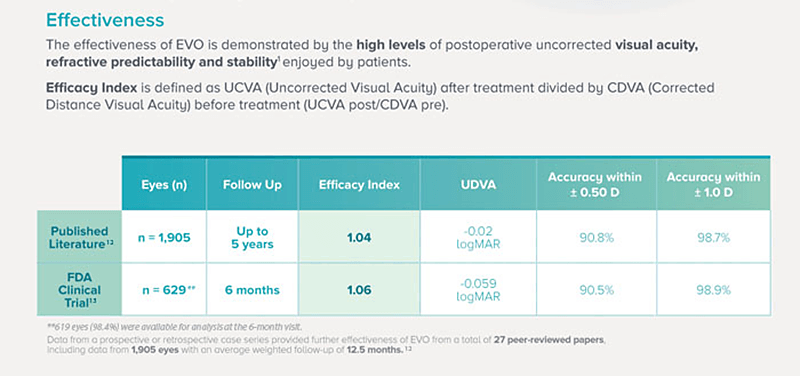 Figure 1. Credit: Image sourced from STAAR Surgical EU EVO HCP Brochure, 2022 STAAR® Surgical Company - MKT-0482-EU-ENG REV. 1 (7,8,9,10)
Figure 1. Credit: Image sourced from STAAR Surgical EU EVO HCP Brochure, 2022 STAAR® Surgical Company - MKT-0482-EU-ENG REV. 1 (7,8,9,10)
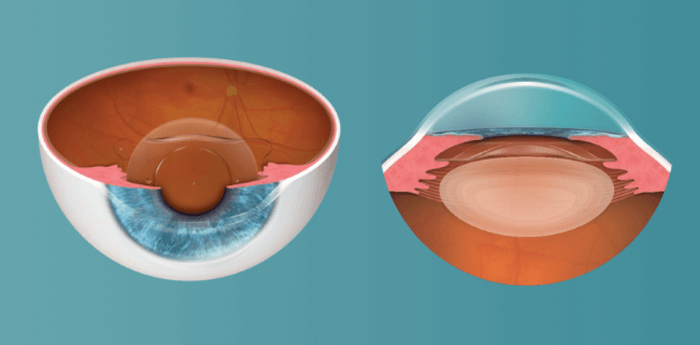 Figure 2: Credit Image Sourced from STAAR® Surgical Company. EVO ICL is a posterior chamber phakic IOL: sitting behind the iris and vaulting the crystalline lens
Figure 2: Credit Image Sourced from STAAR® Surgical Company. EVO ICL is a posterior chamber phakic IOL: sitting behind the iris and vaulting the crystalline lens
Across multiple modes of analysis, from slit lamp exams to anterior segment OCT, it's easy for ophthalmologists to monitor patient outcomes and ICL positioning, says Dr Cummings. The big advantage from a workflow point of view is the procedure's efficiency. For Dr Cummings, the whole procedure can take as little as six minutes. Even treating one eye at a time, with up to a week between eyes, Dr Cummings explains that most of his patients see an incredible improvement in vision immediately following the procedure. Pointing to his colleague Dr Erik Mertens’ short interval bi-lateral surgery preference, Dr Cummings notes that more and more surgeons are choosing to do short interval surgery, thanks to increased confidence in sizing of the lens, the safety that the EVO lens offers (7), the short recovery time and the speed at which patients see visual improvements.
Unsurprisingly then, Dr Cummings reports that of all of the refractive procedures he offers, EVO ICL patients report the highest satisfaction, with crisp, clear vision (4,5), no foreign body sensation, and the peace of mind that comes from knowing that the lens can be removed by a surgeon, if required (though this has never been needed in Dr Cummings’ experience), which also gives flexibility for the future, as the patient ages and becomes presbyopic. Patients also benefit from EVO ICL not inducing dry eye syndrome (1,2) (or STODS), which can be a common risk consideration with surface laser treatments such as LASIK (8).
Why The EVO ICL is a “Game Changer”
High rates of patient satisfaction
Preserves the cornea and crystalline lens
Low rates of adverse events
Outstanding safety and effectiveness
Rapid recovery and outstanding night vision
Use of the EVO ICL has been growing rapidly worldwide, and this is certainly true for Dr Cummings’ own practice, with more cases than ever and with lower and lower refractive errors. As patients hear more about the EVO ICL and talk to friends and colleagues who have experienced the swift recovery and superb outcomes of EVO(7), the demand will only increase according to Dr Cummings and Drs Mertens & Parkhurst. EVO is becoming a key part of surgeons’ refractive offerings all over the world; the future for the EVO ICL looks bright in helping refractive surgeons provide visual freedom from the hassles of glasses and contact lenses, to more and more patients.

Important Safety Information for the EVO/EVO+ ICL
The EVO/EVO+ ICL is indicated for phakic patients 21-60 years of age to correct/reduce myopia up to -20.0 D with up to 6.0 D of astigmatism. Careful preoperative evaluation and sound clinical judgment should be used by the surgeon to decide the risk/ benefit ratio before implanting a lens in a patient with any of the conditions described in the DFU. Prior to surgery, physicians should inform prospective patients of possible risks and benefits associated with the EVO/EVO+ ICL. Reference the EVO/EVO+ ICL DFU available at https://edfu.staar.com/edfu/ for a complete listing of indications, contraindications, warnings and precautions.
Note: indications vary by country, please check your country-specific DFU.

References
- S. Ganesh et al., Matched population comparison of visual outcomes and patient satisfaction between 3 modalities for the correction of low to moderate myopic astigmatism, Clin Ophthalmol, 11, 1253 (2017). PMID: 28740361.
- S.J. Naves et al., “Diadenosine nucleotid measurements as dry-eye scores in patients after LASIK and ICL surgery,” presented at American Society of Cataract and Refractive Surgery (ASCRS) 2012.
- R. Wei et al., Comparison of objective and subjective visual quality early after implantable collamer lens V4c (ICL V4c) and small incision lenticule extraction (SMILE) for high myopia correction, Acta Ophthalmol, (2020). PMID: 32419383.
- E. Martínez-Plaza et al., Effect of the EVO+ Visian Phakic Implantable Collamer Lens on Visual Performance and Quality of Vision and Life, Am J Ophthalmol, 226, 117 (2021). PMID: 33577790.
- GD Parkhurst, “A prospective comparison of phakic collamer lenses and wavefront-optimized laser-assisted in situ keratomileusis for correction of myopia,” Clin Ophthalmol, 10, 1209, (2016). PMID: 27418804.
- M. Packer, The Implantable Collamer Lens with a central port: review of the literature, Clinical ophthalmology, 12, 2427 (2018). PMID: 30568421.
- M Packer, “The Implantable Collamer Lens with a central port: review of the literature,” Clin Ophthalmol, 12, 2427 (2018). PMID: 30568421.
- M Packer. “Evaluation of the EVO/EVO+ Sphere and Toric Visian ICL: Six month results from the United States Food and Drug Administration clinical trial,” Clin Ophthalmol, 16, 1541 (2022). PMID: 35645557.
- M Packer, “The Implantable Collamer Lens with a central port: review of the literature,” Clinical ophthalmology 12, 2427 (2018) PMID: 30568421.
- K. Kamiya et al., ”Posterior chamber phakic intraocular lens implantation: comparative, multicentre study in 351 eyes with low-to-moderate or high myopia,” Br J Ophtalmol, 102, 177, (2018) PMID: 28611132.
- T. Kohnen., “Phakic intraocular lenses: Where are we now?” J Cataract Refract Surg, 44, 121, (2018) PMID: 29587968.
- S. Ganesh et al., “Matched population comparison of visual outcomes and patient satisfaction between 3 modalities for the correction of low to moderate myopic astigmatism,” Clin Ophthalmol, 11, 1253 (2017). PMID: 28740361.
- E. Martínez-Plaza et al., “Effect of the evo+ visian phakic implantable collamer lens on visual performance and quality of vision and life.” Am J Ophthalmol, 226, 117 (2021) PMID:33577790.
- R. Wei et al.,“Comparison of objective and subjective visual quality early after implantable collamer lens V4c (ICL V4c) and small incision lenticule extraction (SMILE) for high myopia correction,” Acta Ophthalmol 98, 943 (2020). PMID: 32419383.
