
Educational content provided by Alimera Sciences.
Introduction The damaging effects of strong light on vision have been common knowledge since Plato’s time. It was not until 1949, however, that sunlight was first used in ocular therapy. In 1960, the development of laser enabled a more precise and effective way of delivering photic energy and, by 1964, the discovery of the argon laser opened the doors to the era of clinical retinal photocoagulation.1
Laser therapy in ophthalmology The different laser therapies used in ophthalmology can be classified according to the ocular tissue lesion they produce:2
- Photocoagulation: here, laser therapy produces thermal lesions by increasing tissue temperature. The increased temperature induces liquid vaporization and protein denaturalization, which, in turn, leads to cellular death. Laser photocoagulation is used in the treatment of diabetic retinopathy and diabetic macular edema (DME).2
- Disruption: in this instance, the laser produces a burst of optical pulses of high power and short duration to ionize tissues. Laser disruption is used during capsulotomy after opacification following cataract surgery, and during peripheral iridotomy to reduce the risk of acute angle-closure glaucoma.2
- Photochemical: this form of laser therapy is used to modify the chemical composition of the target tissue, by altering the molecular composition of previously photosensitized cells. This technique is used in the treatment of exudative age-related macular degeneration.2
- Photodecomposition: in this case, fragmentation of the molecules is caused by the absorption of laser photons at the molecular level. The argon–fluoride excimer lasers used in refractive surgery sculpt the corneal stroma using photoablation.2
Laser therapy in the treatment of DME The use of laser photocoagulation for the treatment of macular degeneration and other macular diseases started during the 1960s.1 According to a recent meta-analysis, it remains a popular treatment option for DME.3 The Early Treatment Diabetic Retinopathy Study (ETDRS) differentiated two laser photocoagulation techniques:
- Focal laser photocoagulation, which produces burns of 50 to 100 µm of moderate intensity, for 0.05 to 0.1 second4
- Grid laser photocoagulation, which produces mild power laser impacts of 50 to 200 µm, for 0.05 to 0.5 second.4
Despite its wide use, the effect of laser photocoagulation on the retina for diabetic retinopathy remains to be clarified.2 Focal laser treatment is believed to directly target the microaneuryms responsible for macular edema,2,3 while different mechanisms of action have been proposed to explain the effects of grid laser treatment in DME, including:
- Destruction of oxygen-consuming photoreceptors2,3
- Decrease in autoregulatory vasoconstriction2
- Reduction of the abnormal leakage area2
- Restoration of the retinal pigment epithelium barrier.2
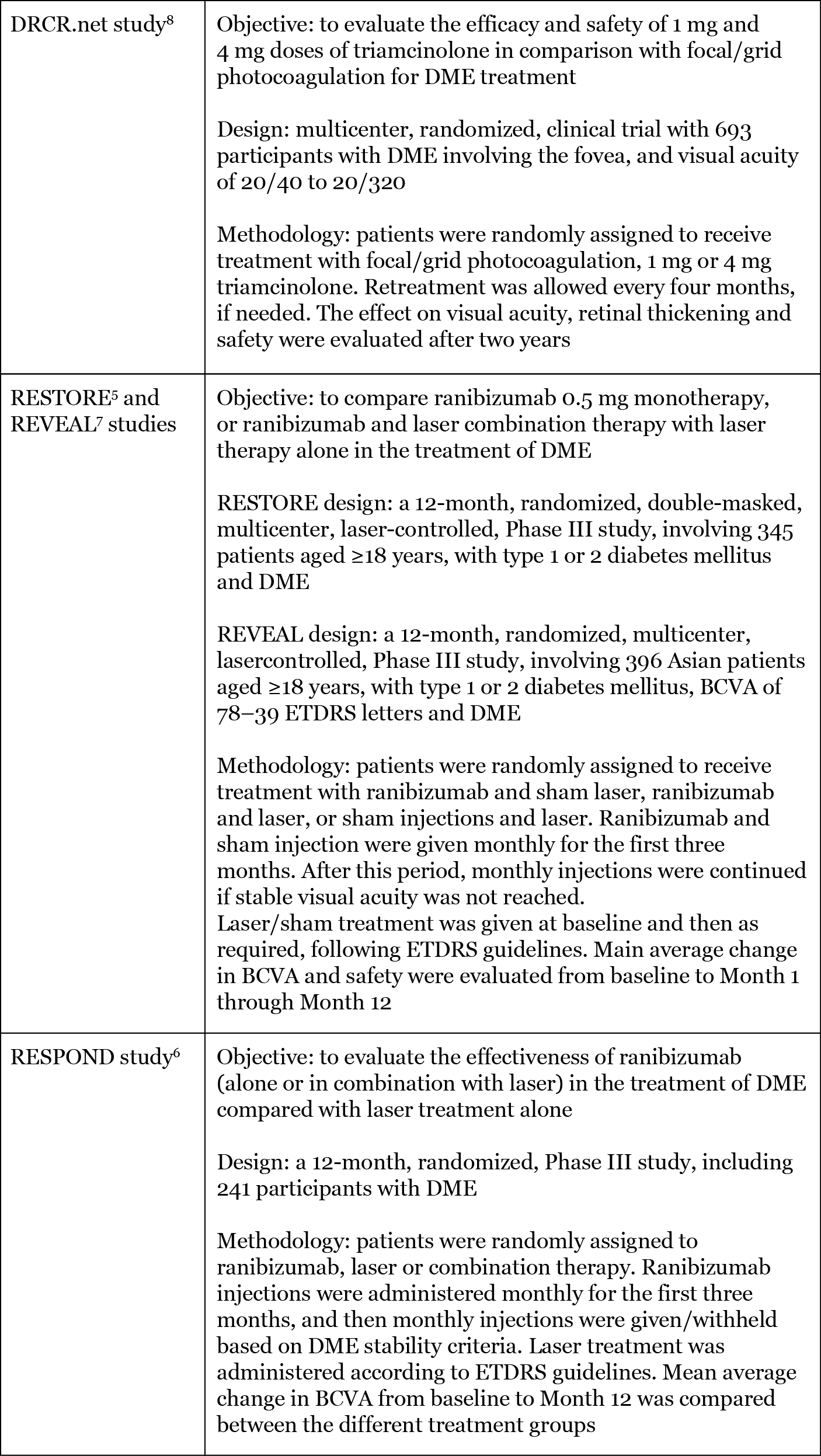
The pros and cons of laser therapy in DME—what can we learn from clinical trials and practice? A number of different clinical studies have tried to evaluate the efficacy and safety of laser photocoagulation, either alone or in combination with other therapies, such as anti-vascular endothelial growth factor (anti-VEGF) agents, in DME treatment. Despite their different design and methodology (Table 1), three of these studies—RESTORE, RESPOND and REVEAL—concluded that ranibizumab monotherapy or ranibizumab and laser combination therapy resulted in greater best-corrected visual acuity (BCVA) improvements at Year 1 than laser therapy alone in patients with DME.5–7 Other studies have evaluated the use of laser therapy and corticosteroids; for example, the Diabetic Retinopathy Clinical Research Network (DRCR.net) study. Results from this study indicated no significant variation between the different treatment groups after 12 months. Furthermore, by Month 16, patients receiving focal/grid photocoagulation showed greater improvement in visual acuity and fewer side effects than those treated with triamcinolone.8 Other studies, such as FAME, included laser therapy as a rescue treatment and, although direct results on laser photocoagulation were not reported, the results presented could suggest that in DME, fluocinolone acetonide (FAc) inserts might provide a valuable addition to laser photocoagulation alone.9 Thus, additional studies are required to further evaluate the outcomes of laser therapy, used either alone or in combination with anti-VEGFs or corticosteroids.
Table 1. Summary of the objectives, design and methodology of the trials evaluating the efficacy and safety of laser photocoagulation, either alone or as a combination therapy.5–9
According to a recent survey, a large proportion of retinal specialists support the use of laser photocoagulation in the treatment of DME.10 Nevertheless, when treating DME, it is important to consider the many potential drawbacks of laser photocoagulation; for example, it can cause several serious adverse effects, including irreversible macular damage11 and retinal cell death.2,12 Occasionally, reductions in visual acuity have also been reported following photocoagulation therapy due to the enlargement of the laser scar.12
Novel treatment modalities—the role of laser photocoagulation in the 21st century Recent advances in the development of laser therapy have resulted in novel DME treatment modalities. A new form of laser therapy, subthreshold micropulse diode (SDM) laser photocoagulation, appears to be as effective as standard laser photocoagulation and reduces the risk of serious complications.3,13 SDM laser produces a subthreshold laser micropulse, using an 810 nm diode laser, thereby reducing the damage to ocular tissue.2 The mechanism of action of SDM laser is still unclear, but it is believed that it may selectively target the retinal pigment epithelium, inducing changes in cytokine levels.13 Another new approach to macular laser therapy is mild macular grid (MMG) laser photocoagulation, where the laser burns are targeted to the entire macula (including unthickened retina). MMG laser burns are lighter and more diffuse than those produced by conventional laser photocoagulation, and microaneurysms are not directly photocoagulated.2 The new laser photocoagulation techniques described have the potential to replace conventional laser photocoagulation; nevertheless, at present, not enough evidence-based data are available, and further studies are required if either of these techniques is to lead to a paradigm shift within laser photocoagulation.2
Conclusion Laser photocoagulation continues to play a key role in the treatment of DME, particularly given recent advances, such as SDM laser. However, the advent of other DME treatment options, such as intravitreal anti-VEGF and corticosteroid therapies, offers alternative, as well as complementary, treatment modalities to laser photocoagulation.
Paolo Lanzetta is Professor and Chairman of the Department of Ophthalmology at the University of Udine, Italy, and Founder and Scientific Director of the Istituto Europeo di Microchirurgia Oculare—IEMO, Udine, Italy. His main activity areas are laser applications in ophthalmology; diagnosis and treatment of vitreous, retinal and macular diseases; and cataract surgery. Professor Lanzetta is actively involved in retinal clinical research and is currently an investigator in many international, multicenter, clinical trials on photodynamic therapy (PDT), anti-angiogenic, and new drugs, and delivery systems. With surgical experience in anterior and posterior segment procedures and laser treatments, Professor Lanzetta has given over 350 presentations at national and international meetings. He is a member of numerous professional societies, including ARVO and the Macula Society. As well as publishing over 170 original articles, Professor Lanzetta is a scientific reviewer for many journals and serves on the Editorial Board of the European Journal of Ophthalmology. Valentina Sarao is a retinal physician at the Istituto Europeo di Microchirurgia Oculare-IEMO (Udine, Italy). She received her medical degree from the University of Udine, where she also completed an ophthalmology residency. She is mostly interested in advancements in laser technology, and in diagnosis and treatment of retinal and macular pathologies. She is actively involved in retinal clinical research, and is currently an investigator in many international, multicenter clinical trials on anti-angiogenic and new therapies, and delivery systems. She also regularly attends national and international symposia on these topics as an invited speaker.
Look out for DME content developed by Alimera Sciences on this website throughout 2015. We hope it supports your knowledge of DME, and if you would like to contribute material for publication, please send your materials to dmecontenthub@hayward.co.uk, we’d be very pleased to consider your contributions.
REFERENCES
- DV Palanker et al., “Fifty Years of Ophthalmic Laser Therapy”, Arch Ophthalmol, 129, 1613–1619 (2011). PMID: 22159684
- P Romero-Aroca et al., “Laser treatment for diabetic macular edema in the 21st century”, Curr Diabetes Rev, 10, 100–112 (2014). PMID: 24852439.
- C Mathew et al., “Updates in the Management of Diabetic Macular Edema”, J Diabetes Res, 2015 (2015). PMID: PMC4423013.
- Early Treatment Diabetic Retinopathy Study research group, “Photocoagulation for Diabetic Macular Edema. Early Treatment Diabetic Retinopathy Study Report Number 1”, Arch Ophthalmol, 103, 1796–1806 (1985). PMID: 2866759.
- P Mitchell et al., “The RESTORE study. Ranibizumab Monotherapy or Combined with Laser versus Laser Monotherapy for Diabetic Macular Edema”, Ophthalmology, 118, 615–625 (2011). PMID: 21459215.)
- A Berger et al., “A Canadian 12-month, PhIIIb study of ranibizumab combination or monotherapy in visual impairment due to diabetic macular edema: preliminary analysis (“RESPOND”)”, Can J Diabetes, 37, S48, abstract 129 (2013).
- T Ishibashi et al., “The REVEAL study: Ranibizumab monotherapy or combined with laser versus laser monotherapy in Asian patients with diabetic macular edema”, Ophthalmology, 122, 1402–1415 (2015). PMID: 25983216.
- Diabetic Retinopathy Clinical Research Network, “A Randomized Trial Comparing Intravitreal Triamcinolone Acetonide and Focal/Grid Photocoagulation for Diabetic Macular Edema”, Ophthalmology, 115, 1447–1459 (2008). PMID: 18662829.
- PA Campochiaro et al., “Sustained delivery fluocinolone acetonide vitreous inserts provide benefit for at least 3 years in patients with diabetic macular edema.” Ophthalmology, 119(10), 2125–2132 (2012). PMID: 22727177.
- S Mansour, “What is the current role of laser therapy in the management of DME?” Retina Today, 68–70 (April 2015). Available at: http://retinatoday.com/2015/04/what-is-the-current-role-of-laser-therapy-in-the-management-of-dme. Accessed September 10, 2015.
- F Boscia et al., “Is macular laser indicated in era of anti-VEGF therapy? No, not anymore.”,
- P Romero-Aroca, “Is laser photocoagulation treatment currently useful in diabetic macular edema?”, Med Hypothesis Discov Innov Ophthalmol, 4, 5–8 (2015). PMID: 25861668.
- P Lanzetta. Debate II: Is macular laser indicated in era of anti-VEGF therapy? Yes, sub-threshold laser.
Founded in 2003, Alimera Sciences researches and develops innovative vision-improving treatments for chronic retinal diseases, such as diabetic macular edema (DME), dry age-related macular degeneration (AMD), and retinal vein occlusion. In 2015, Alimera Sciences partnered with The Ophthalmologist to facilitate the publication of independently created educational content surrounding DME, a serious retinal complication associated with diabetes, which is increasing in incidence with the increasing prevalence of diabetes worldwide. Published content will include articles ranging from basic science and disease processes to overviews of clinical data, different surgical procedures, comparisons of treatment options, and practical advice for managing diabetic patients. With a commitment to honesty, integrity, responsibility, candor, and trust, Alimera Sciences intend to provide educationally focused content to healthcare professionals across a wide range of topics in DME in order to both increase disease awareness and understanding, and to help improve patient outcomes. UK-ILV-MMM-0355 Date of preparation: August 2015 enquiries@alimerasciences.com
