The RayOne EMV enhanced monofocal IOL platform is an important addition to the armory of ophthalmologists in presbyopia management, according to Andrew Turnbull, consultant ophthalmologist and cataract service lead at University Hospitals Dorset NHS Foundation Trust, Bournemouth, UK. “What we are seeking is spectacle independence at all distances and maximum visual quality. And that is the major attraction of RayOne EMV; it has increasingly become my standard lens for private patients,” he said. “For those who don’t have access to a laser refractive practice or complex diagnostics, I think RayOne EMV has an important place for someone who is embarking on a journey into premium lens practice.”
Turnbull said that, because the EMV behaves very much like a standard monofocal lens, it does not have the problems that may arise with trifocal lenses, adding, “It gives me more confidence in proposing a given strategy to a patient.”
Another advantage of RayOne EMV, according to Mr Turnbull, is that it does not require too much preoperative discussion with patients. “I will spend 10 –15 minutes discussing refractive targeting. I will spend a bit more time if we are going down the trifocal route,” he noted at an advanced technology IOL webinar organised by Rayner.
Allon Barsam, director and founding partner at OCL Vision and the world’s first implanter of RayOne EMV, said RayOne EMV nicely bridges the gap between the capabilities of a standard monofocal and a trifocal lens.
“One of the nice things about RayOne EMV is that you can use it in scenarios where it would be inappropriate to use a trifocal lens. I have probably inserted 300 RayOne Trifocal IOLs but I have used a similar number of the EMV as well.” Barsam said that RayOne EMV has become his “go-to” lens.
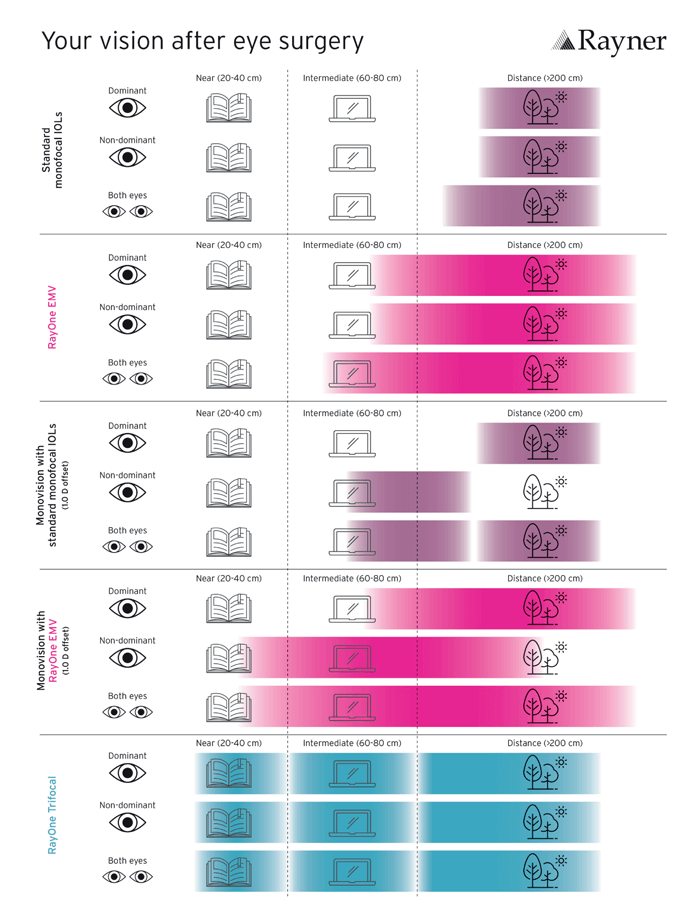
“I start off with the premise that this is the lens that I would use in my patients, unless there is a reason not to. The main reason not to use this lens, in my opinion, is if a patient comes to me with the desire to be totally spectacle independent. With a monovision scenario you can achieve N5 [J3] or N6 [J4]. You could – with enough monovision – even achieve N4 [J2].
“If a patient wants to do large amounts of reading, I feel a trifocal IOL is better – but most of my patients do not request that. Most of my patients want to be independent of glasses for distant activities and intermediate activities, such as using their computer screens. Then there is also what I call ‘social reading,’ which is not at the level of N4 [J2] or N5 [J3], where patients want to be able to see the menu in a restaurant or to be able to see their phones or watches. RayOne EMV gives you the opportunity to offer patients independence from glasses for almost everything. I think it is a great entry point to making patients really happy with very minimal risk.
“How much independence you give them depends on how much they want and how much monovision they want. If they are very easy going and happy with glasses, I would target plano in the dominant eye and -0.25 D to -0.5 D in the non-dominant eye. If patients want independence from glasses but I feel uncomfortable about using a trifocal lens, I think RayOne EMV is a better option because it doesn’t give them glare, halos, or dysphotopsia. My trifocal lens usage has reduced a little bit, but my overall advanced technology lens usage has gone to almost 100 percent because I cannot really think of scenarios where a patient would not want the RayOne EMV lens or you wouldn’t want to use it. There is a pricing consideration, but outside of that I do not see any downside,” he said.
Barsam said surgeons and clinicians need to consider how the language and optical information with which they are familiar differs from the mindset of a patient when they consider using RayOne EMV.
We might think that quality vision is the best that can be achieved with glasses, whereas for a patient what they describe as quality of vision is basically being satisfied with their vision – which includes the range of their vision. What is very difficult for patients to conceive is that, if you use a standard monofocal lens and the patient is pseudophakic, they only have a focus at that one particular point, which in my opinion is not good quality vision.
“Natural quality vision is where there is a natural range of vision – and that is what RayOne EMV provides. In terms of functional vision, which is the patient feeling that the vision is natural, this lens does provide better quality of vision and therefore it costs a bit more than other lenses.
“We may feel that we have to impart all of our knowledge to our patients, but they will not understand the optical intricacies of everything that we know as ophthalmologists. There is a lot of data now showing the benefit of RayOne EMV without significant detriment. In terms of the cost, it is less than they spend on glasses and I don’t find the price point to be an issue for patients.”
On the issue of pricing, Turnbull said that, in his opinion, it is the job of the refractive surgeon to identify the lens that best suits the patient to achieve the best functional outcome. As such, his private patients pay the same regardless of whether they are receiving a standard monofocal, toric or enhanced monofocal lens.
“It is about finding the right fit. Just because they have astigmatism or a bit more spherical aberration than normal, I don’t think that patients should need to pay extra. That is my approach for selfpaid patients. For insured patients (who must pay out-of-pocket for advanced technology lenses) I set out the fact that cataract surgery is not just about removing the cataracts. There is an opportunity to improve the patient’s overall quality of vision and their dependence on glasses,” he said. “A lot of my patients are often not aware of that, so it is a case of educating them that there are other options and finding out what options are going to be the best for them.”
Barsam said that improved patient education was important, and he also suggested a change in terminology with patients from “premium lenses” to “non-standard” or “advanced technology lenses.”
“The more patients are educated by community optometrists and by each other and by what they learn in their consultations with ophthalmologists, the better. It is a reality in the developed world that advanced technology lens usage happens less frequently than it should – and fewer patients get these lenses than we know would benefit from them. We should also consider the fear of change.
“Change is uncomfortable and for an ophthalmologist, when it is your surgical patient and your practice, the instrument in which change needs to apply may take a lot of courage. It is so much easier to do what you have always been doing. You may always have been using standard lenses and feeling comfortable with that. For those of us with busy private practices, I can say they are busy because our patients tell their friends that they have good vision. If they did not have good vision, they would not recommend us.”
In conclusion, Barsam said that he is happy to tell surgeons that, if they try RayOne EMV, they will like it. “It is one of those lenses where you get a lot without having to give up very much.”
