
I never planned to create a business with ophthalmic surgery training models – the SimulEYE line of ophthalmic surgical training models happened almost by accident. In fact, it started as a hobby, but when I found that I had a knack for modeling, it became a passion. And when I saw how people reacted to the models, and how much they were appreciated, I began to get a real joy out of it. Nevertheless, turning a hobby into a business has been challenging; obligations to my practice and my family always came first, but InsEYEt (the LLC behind SimulEYE) took up any other time that I wasn’t sleeping... Now, the company has taken on a life of its own, and all I can do is hold on tight and see where the ride takes me!
Mother of invention
It all began when I took time out of hands-on surgery during my LASIK-only residency with Dr. Howard Gimbel in Canada. The Canadian government allotted all cataracts to Canadian surgeons, and so, although I learned a tremendous amount from watching Howard, I couldn’t actually do any cataracts myself. In fact, I didn’t perform cataract surgery for a year, so when I returned to Beverly Hills in 2001, I struggled with some of the steps of cataract surgery, particularly the continuous curvilinear capsulorhexis (CCC) technique. I knew I needed to practice and refine my competencies – and fast. But how? At first, it seemed there was no quick way to make my life easier. I’d found some suitable plastic film, but couldn’t see how to mount it under tension to make an acceptable model of the eye. One day, however, when I was checking out of a store, I saw some silly putty on the shelf – and that was the ‘aha’ moment! I took the putty home, and discovered that by wrapping the film around it and squeezing I could make it as dome-shaped as I needed. Furthermore, I could cause the tear to run out and practice rescuing the CCC. Doing multiple practice sessions with this model before surgeries helped me very quickly regain my skills. I didn’t know it at the time, but that simple prototype was the basis of the SimulEYE models. A couple of years later, at the ASCRS meeting in 2005, I presented a video of my model. I wasn’t trying to sell it – I just wanted to make it available to residents to benefit them and their patients. But I found that residents weren’t interested in making models; they wanted an off-the-shelf kit. So I made one. Next question: how to distribute it? I showed it to some of the bigger companies, and they loved it – but not always in the way I expected. For example, the head of Bausch and Lomb said, “This is a million dollar idea, but we’re not interested.” He thought I was trying to sell him the entire concept, when I just wanted him to buy the kits from me and distribute them to residents. In any case, those discussions were torpedoed by the Sunshine Act, which prevented pharma from giving out freebies. Even free pens were off-limits, so my surgical training models were definitely not going to reach end-users by that route.It was a frustrating time. Maintaining patents is a costly process, and I couldn’t help wondering if it was all worth it. But then I got an email from a company called Truevision 3D. The folks there had seen my patents, and wanted to use my system to demonstrate their technology at trade shows. Truevision was located in Santa Barbara at the time, only an hour away from my house, so I went to see them. It turned out that they needed a model eye to go under their 3D video scope. I said that the hand-held model I had developed wouldn’t be adequate for their purposes (way too amateurish for doctors!), but I’d help them if I could. However, making a new model eye isn’t easy, so I spent days searching hardware stores for parts that I could use to improve the existing device. I tried all kinds of things – sprinklers, door-stops, pot magnets – and eventually constructed something that had enough weight for stability and that could hold the film under tension. And Truevision loved it! After that, things really started taking off. Truevision would demonstrate their videoscope at trade shows, people would ask where they got the model eye, and I would get call after call. So I formed insEYEt, LLC, to deal with the demand. We started with SimuloRhexis (Figure 1), a model for CCC training, which has evolved tremendously over time. One of the first people to try it was Kevin Miller, who runs a wet lab course for UCLA residents. And soon he was asking for other models; one time, he asked for a YAG capsulotomy training model to support Lumenis demonstrations – only three months before the course started! I said I would do it, even though I had no idea how. And I did, although it was a real scramble.
New model army
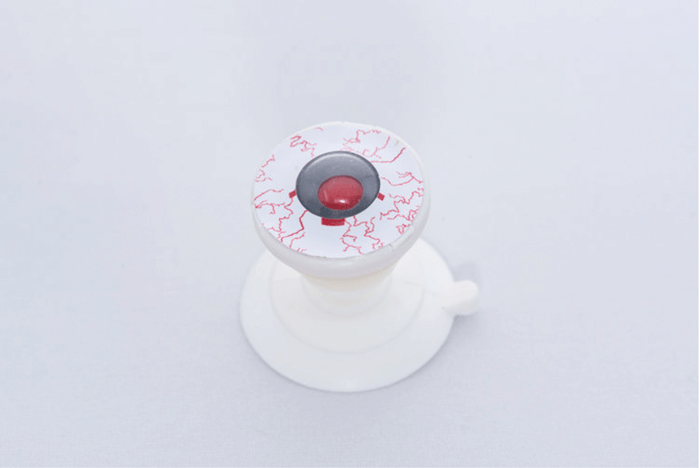
From there, more and more opportunities came along, and I developed model after model. At InsEYEt, we coined the name SimulEYE to cover our growing range – models not just for rhexis, but for YAG (Figure 2), for laser peripheral iridotomy (LPI; Figure 3), for selective laser trabeculoplasty (SLT; Figure 4), and so on. Today, we have 16 models, four of which are for MIGS training. But SimuloRhexis was our first model, and it remains fundamental – all residents should use this. The YAG laser models for SLT and LPI are also very important; I know this from experience, because I’ve had residents on their first laser operation ask me things like what settings to use, and how to change the power! You really shouldn’t be asking those kinds of questions when you have a patient seated at the laser.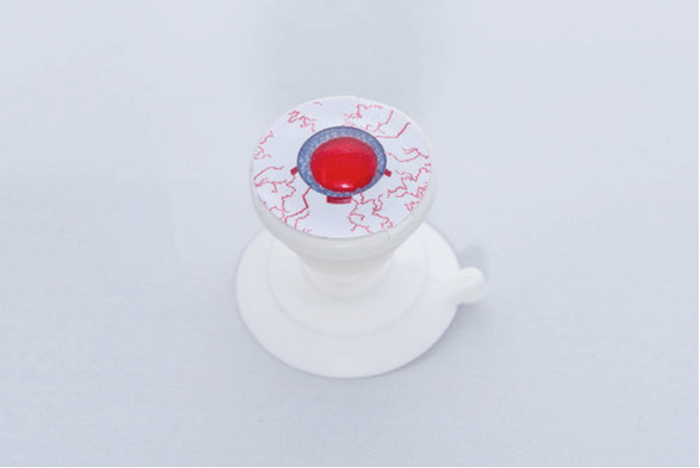


Our training model for ring implants was also a very significant product innovation. We started working with MicroSurgical Technology (MST) about four years ago. I’d made a prototype model for Malyugin ring implant training, and showed it to the rep at the MST booth. She immediately pointed to the guy next to her –who turned out to be Larry Laks, the head of MST! And now all the MST reps have a Small Pupil SimulEYE (Figure 5) for teaching Malyugin ring procedures. The model helps MST to train doctors properly, and that helps prevent complications, such as intraoperative floppy iris syndrome, which can arose from medications like Flomax. The next additions to our portfolio included the SimulEYE Femto model for Alcon LenSx training. The impetus for this product came from my LenSx training session, as the model eye we used was a complete horror show – completely unrealistic scanning and docking. I knew I could do a better job, so I made some prototypes and then met up with the LensX engineers and showed them what I’d done. They loved the concept, and realized they needed something better than they had and that I could give it to them. So I developed the prototypes into a LenSx eye – but just as I finished the model, they introduced laser autoregistration! Obviously, they weren’t going to re-write their software to match my SimulEYE model; I would have to make my model compatible with their software. Consequently, I went back to the drawing board, and we modified our materials to fool the laser so that the autoregistration features would work. The end result was a LenSx model that you can dock and scan, where everything auto-registers and you can use the software as normal. Furthermore, you can hit the button and see an actual treatment happening – bubble patterns, capsulotomy, lens fragmentation, corneal incisions – all in one model!
Making a new SimulEYE mostly involves finding new materials and trying them out; I may not have an engineering background, but I think I now have a Master’s in trial and error! It also helps to be a practicing ophthalmologist, as knowing how ocular tissues look and feel is invaluable when you are modeling them. Even so, SimulEYE development was awkward at first; I didn’t even have a standard housing to hold the different components of a model – instead, I’d pay 50 cents at a candy machine and use the container as a housing. But things have gotten much easier over time. Today, we have molds for the housing and other standard components, and that has really accelerated the development of the SimulEYE portfolio. The housing and the externals are very similar for all of our models; for example, they all use the suction-cup base, because it both confers stability and permits eye movements in a self-supporting platform which does not require a head model. The models mainly differ with regard to the interior – the iris plane, the materials used, whether we have a flexible iris, whether we have a capsular bag, whether we use gels or simulated vitreous, and so on. We outsource housing manufacture, but the internal parts are fabricated in-house and then put into each model manually. At present, we 3D-print our prototypes in the initial design phases, but use steel injection molds for the final products; however, our manufacturing model may incorporate 3D-printing in the future, if it improves. We’re keeping an eye out (no pun intended) for technology developments, and we will change our manufacturing process, if it becomes appropriate to do so. In all cases, we ensure manufacturing costs are controlled. And that’s how we can sell models, such as the LenSx SimulEYE, for only $40! Even our higher-priced eyes are extraordinarily good value: thus, the ABiC iTrack (Figure 8) is priced at $200, because the incorporation of channels makes it a more complex item; however, it can be used multiple times, so it still works out at about $40 per procedure. We’ve always tried to find a balance between the price for our corporate partners and one that would be affordable to residents with limited budgets.


The Ophthalmologist overheard Steve Safran talking with Stuart Stoll at Cataract Surgery: Telling It Like It Is 2018. “Thank you very much for making this event a success. Your simulated eye is a fantastic model and showed itself as such today [...] I didn’t have a model in mind when I moved towards doing a wet-lab. Then somebody gave me a SimulEYE that they’d received from a course they’d taken. I played with it and liked what I saw.” Stoll’s reaction? “We get these kinds of endorsements all the time! But hearing positive feedback is really rewarding – when a well-known ophthalmologist gets excited about your product, you know you’ve done well.”
With the momentum of the SimulEYE Femto sales, I rented a commercial facility, and InsEYEt really started moving. The SimulEYE Femto isn’t our only model popular with industry; many others have proved tremendously helpful for companies selling products in their respective fields. For example, when Alcon re-launched the Ultrasert preloaded injector, all their reps used our Aphakia model (Figure 6) to demonstrate Ultrasert lens delivery. In fact, at the AAO meeting in 2017, I got talking to a rep who was using our Aphakia eye model, and when he realized that I was the one who developed it, he lit up and told me how much the sales team loved it. I get that all the time!
