The development of the Zepto capsulotomy device is more than a little unconventional: ten years ago, two newcomers to the field (us), with very little funding, no experience of medical device development, and no track record in ophthalmology, decide to work together to create a new capsulotomy device. From that background alone, you’d be forgiven for thinking it was a long shot. But since that lightbulb moment, we’ve come a long way – the Zepto capsulotomy device received a CE mark in 2015, and our work was presented at the 2015 Ophthalmology Innovation Summits in San Diego and Las Vegas, and the 2015 Ophthalmology Futures Forum in Barcelona. And it all began with micromechanical knives…
Gizmos and glaucoma
Before we met, Chris had worked at IBM for 10 years, designing hard disc drives, before returning to school to undertake a PhD in material science at the University of California, Berkeley. The research was fascinating; it focused on microelectromechanical systems (MEMS), which are made on silicon wafers using integrated circuit processes to create micromechanical devices. Because working for such a large company no longer appealed to Chris, after graduating, he started his own sole proprietorship creating nifty little gizmos, such as microknives, for the local professors. David, who was using microknives to perform surgery on individual nerve cells growing in petri dishes, became a customer. It wasn’t long after meeting that we decided we wanted to work together to develop a practical medical device.At first we focused on glaucoma – our idea was to create a device that would enter Schlemm’s canal and cut the wall to enter the trabecular meshwork, creating another outflow pathway. But although we worked on the idea for some time, we didn’t meet with much success. We were relative newcomers to the field, and at the time a lot of MIGS companies were being launched and netting funding, and were much further ahead than us. In 2008, venture capital funding was also very scarce, and we had no luck getting our idea funded. So, we were left scratching our heads. But all along we’d had a second idea: a capsulotomy device. We knew there was a need for a miniature device that could create a capsulotomy. And we felt this was something we could develop ourselves, with lower costs and a higher chance of succeeding. We had this conversation one morning, and by that very afternoon we had switched track and begun work on the new device – with just the two of us, we could move very quickly.
Ignoring the hype
Creating a capsulotomy device wasn’t without its own challenges – in 2008, the first femtosecond laser-assisted capsulotomy was performed in a human eye, and the hype around these lasers was immense! But luckily, we were naïve enough to imagine that two guys working together in a garage (so to speak) would be able to make headway against these well-funded femto companies. In all likelihood, no one would have given us a chance at that stage – if you read what was being published in the trade journals, everyone was saying “this is the future, we’ve got it solved.” But we knew a lot about the mechanics of cutting small things like thin membranes, and we realized that the lasers had a lot of drawbacks. We had our own, totally different approach, which didn’t involve the same costs, or bulky equipment, and which held its own particular benefits. When femto started to dominate the news, when almost everybody was talking about it, this actually kept us going – we were able to ignore all the noise and just believe in the project. And it paid off; people are now recognizing that there are drawbacks with femto, from costs to clinical disadvantages.Cephalopod capsulotomy
So despite the advent of laser capsulotomy, we kept working on our device. With no money for fancy lasers or expensive equipment, we knew we had to keep it simple. In some ways this became an advantage, as it forced us to be much more creative than we might have otherwise been. One of our first tasks was to look at the literature, to see what methods had been tried in the past – one method which is in some ways similar to ours is the Fugo Blade. But this device involves using a probe tip that has to be moved in a circular fashion, it makes success very dependent on the surgeon’s skill. We aimed to design a device that wasn’t limited by this issue. Initially we tried mechanical methods, in the same vein as the microknives we’d both worked with before, but it soon became clear that this wouldn’t work. Our next idea was to use a tiny micro spot welder that was made from gold wire, just 100 µm in diameter. We tried it with a lens from a rabbit eye, held it up to the lens ran a current through the fine gold wire by discharging a 20 µF capacitor through it. It made a cut, so we knew it would work. Having worked in a microenvironment before, we knew that we had to use a short pulse to avoid collateral damage to neighboring tissue, so the energy density was important, and had to be highly localized in both space and time. There also had to be a force pushing the membrane against the electrical cutting element. When it came to force, we took a cue from squid – their use of suction cups to create a complete force circuit and grip onto things is both elegant and uncomplicated. We wanted a similar suction cup gripping the surface of the lens, pulling it into the cutting element, so that the capsule is under mechanical tension exactly on the circle you want to cut. This means there’s no force going anywhere else in the eye, and you’re not pulling the zonules, or putting other areas under strain (see video below) – the force circuit is entirely contained within the suction cup and the front of the lens. We built some prototypes to test our idea, and they worked very well! We needed some images to demonstrate what our device could do, so Chris went and paid a fee to the University of Berkley Electron Microscopy Imaging Center to take some scanning electron microscope images to demonstrate what our device could do.Funding firsts
Developing and obtaining proof-of-concept for this idea was critical – if we had tried to approach institutional or venture capital funding before that point, it would probably have been unsuccessful (this was the time of all the hype around femtosecond lasers). So this was a project that required a lot of initial investment and hard work from just the two of us. And when it came to finally obtaining some funding, we were in luck. We developed our proof-of-concept device using rabbit eyes, primarily because they were cheap and convenient to use. But it’s also known that the rabbit capsule is similar to that of an infant, in that it’s very elastic. It was this initial focus on pediatric applications that helped us to secure our first grant. The National Eye Institute (NEI) in the US is particularly interested in developing ophthalmic devices proven to work in pediatric patients, because of the lack of devices commercially available that are suitable for this patient group. The result? A lot of children consigned to having instruments used in their eyes that were developed for adults – not an ideal situation. This inspired us to approach them with our idea for a device that would work particularly well for pediatric capsulotomies. When we showed them our data, they were interested, and we netted our first grant support, helping launch us onto a faster trajectory. Ultimately, we were able to get a whole series of Small Business Innovation Research (SBIR) grants awarded to our company, and several other government grants too. This allowed us to proceed with our project without needing institutional or venture capital investors.From proof to prototype
Having some funding accelerated development, and we were able to move from a device that demonstrated our cutting method, to a working prototype of Zepto that could be used surgically (see video “Zepto – How it Works”). It satisfied all of our initial design goals: a small incision device that could expand to the appropriate size, a circular cutting element, and the use of suction to create a perfectly round capsulotomy. And we realized Zepto had another feature we hadn’t planned for: transparency. Once we had our prototype, we realized that the thin-walled suction cup we were using essentially disappears when you put it into the eye. You could actually use the device for visual centration during the procedure. When we were working on Zepto, we were looking at the engineering aspects of making a circular cut, but we didn’t realize that ophthalmologists had trouble keeping a pupil dilated or centering the visual axis. This was a completely serendipitous discovery.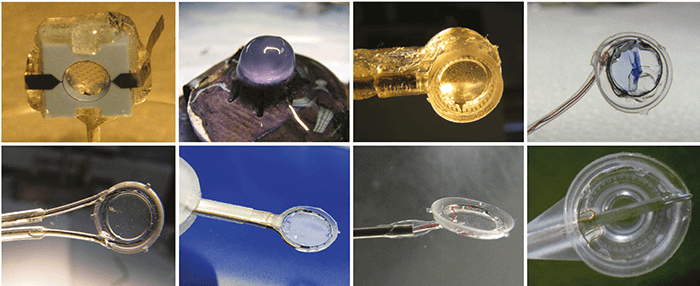
Bringing in the business experts
Now that we had our surgical prototype, we knew we needed to find experienced management to help us. We simply didn’t have the know-how to gain regulatory approval – if we’d tried to do it ourselves, we would likely have been foundering and wasting a lot of money making avoidable mistakes. So we started networking, making contact with people who could potentially come on board. John Hendrick was one of the names that came up, and we made an appointment to see him. John told us he was interested, but didn’t yet know if he would be available to work with our company, Mynosys, as he was waiting for the results of a clinical trial at the company he was working with at the time. He told us to call in four months and he’d have an answer, and we did. Luckily for us, he was free, and realized the potential of Zepto (see “Going for Gold” below). Having John and his team to help us navigate regulatory approval has been fantastic – John himself was previously Vice President of Operations at Allergan Medical Optics, and actually led the team that developed the first foldable silicone IOL, so he’s very familiar with cataract surgery. In fact he told us that back in those days he led a team that tried to develop a capsulotomy device, but it didn’t work out. The idea stayed with him, and when he saw the videos that Chris and I had brought to our first meeting, the light bulb came on in his head and he realized that – aha! – this might actually be it, what he had been trying to do so many years ago, and what other people had been trying to do in the years since. So now we’re transitioning our product towards production, and we’re very lucky to have John’s expertise – he is a true master of the art of contract manufacturing. He understands the margins and timeframes, and has an amazing network of contacts to draw on. He knows where to go, and who to see, and these are things it could have taken us a very long time to figure out. Working with an expert helped us side-step a lot of mistakes, and the progress we’ve made in the last two years has been phenomenal. Admittedly, Mynosys remains a very, very small company in comparison to other medical device manufacturers; we have just seven employees. But our incredibly efficient and highly experienced team has seen us do more with so much less – achieving more in just 24 months than many other projects manage with much bigger budgets, and longer time frames.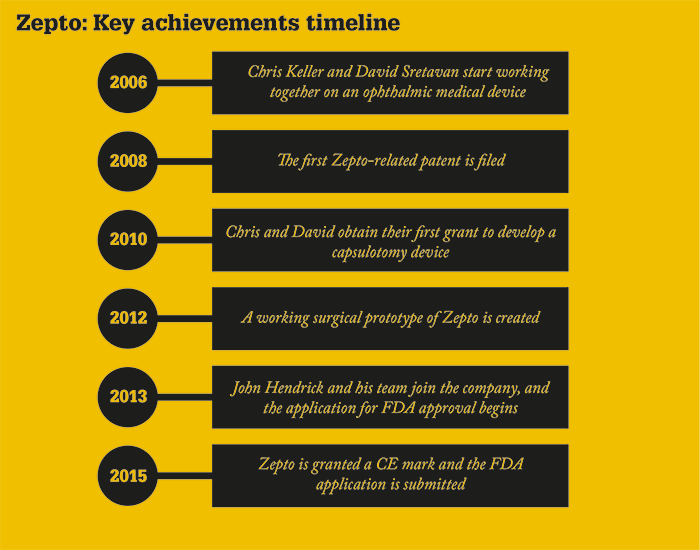
The future
As Zepto heads towards the market, we’ve shown the device to many surgeons who have been overwhelmingly enthusiastic, and very helpful with their feedback – Kuldev Singh even suggested the name! But the facts are that it’s inexpensive, provides what we think is a better capsulotomy than can be achieved by hand or by laser, and can let you do something that neither of the other techniques can do: perioperative centration on the visual axis. We don’t know for sure if or how Zepto will disrupt the femtosecond laser market, but given the proposition, you have to think that, once launched, it will make a very big impact indeed.John Hendrick, President and CEO of Mynosys Cellular Devices
