
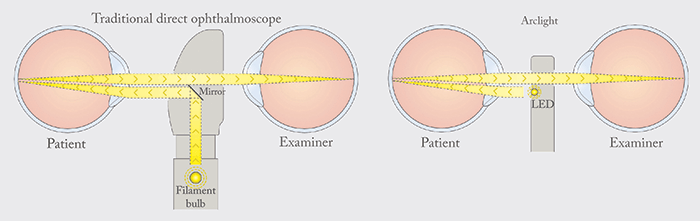
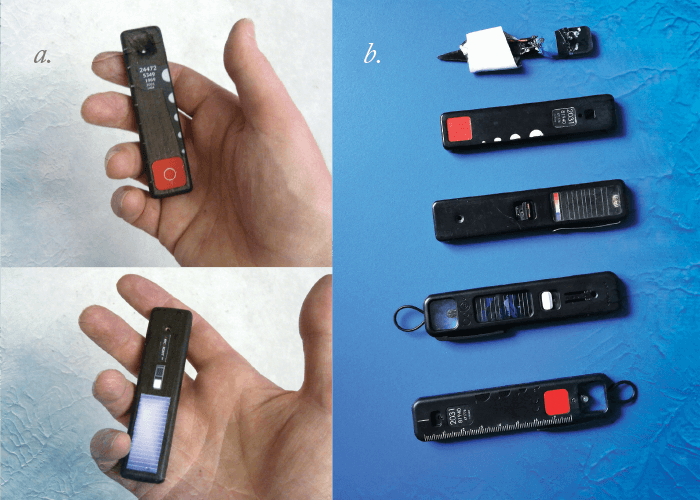
I’ve always been amazed by ‘pound shops’ – how can things be manufactured, packaged and shipped around the world with middlemen and mark-ups and still be so cheap? Combining a knowledge of optics and electronics, I figured I could create something low cost too. With zero thoughts about business plans or world blindness – it was just a fun weekend challenge to simplify the ophthalmoscope, making it lighter, cheaper, and maybe even better. The laws of direct ophthalmoscopy optics don’t change, so my first approach was to strip out almost every feature on scopes that are designed to last a career, so that all it could ‘do’ was ophthalmoscopy and nothing else. LEDs are bright and very small, and can be mounted directly below the sight hole facing the patient; removing the mirror and optics allows the device to have a slim profile, letting users hold it close to both their own and the patient’s eye for a clear dust-free view (Figure 1). The first prototype – which took 10 minutes to make – was a plastic ice lolly stick with a hole and an LED. I tested it on a young cat, then a dog, a child, a middle-aged person, then a pensioner – in order of ascending eye and pupil viewing difficulty. A wooden size and shape mock-up followed. With the basics sound, better prototypes came, adding in solar power and USB charging (Figure 2). Later, I fitted a loupe lens, realizing that with a bit of adjustment, it made a highly maneuverable otoscope.
I’ve always been amazed by ‘pound shops’ – how can things be manufactured, packaged and shipped around the world with middlemen and mark-ups and still be so cheap? Combining a knowledge of optics and electronics, I figured I could create something low cost too. With zero thoughts about business plans or world blindness – it was just a fun weekend challenge to simplify the ophthalmoscope, making it lighter, cheaper, and maybe even better. The laws of direct ophthalmoscopy optics don’t change, so my first approach was to strip out almost every feature on scopes that are designed to last a career, so that all it could ‘do’ was ophthalmoscopy and nothing else. LEDs are bright and very small, and can be mounted directly below the sight hole facing the patient; removing the mirror and optics allows the device to have a slim profile, letting users hold it close to both their own and the patient’s eye for a clear dust-free view (Figure 1). The first prototype – which took 10 minutes to make – was a plastic popsicle stick with a hole and an LED. I tested it on a young cat, then a dog, a child, a middle-aged person, then a pensioner – in order of ascending eye and pupil viewing difficulty. A wooden size and shape mock-up followed. With the basics sound, better prototypes came, adding in solar power and USB charging (Figure 2). Later, I fitted a loupe lens, realizing that with a bit of adjustment, it made a highly maneuverable otoscope.
Throughout the process, I’ve had to be a bit of a “jack of all trades” – learning computer-aided design, injection molding, ultrasonic welding, as well as web and graphic design. With no committees, I could be nimble – and use a common sense “keep it simple” mantra with engineering. The decision to move from prototype to product came from listening to the wisdom of ophthalmologists, such as John Sandford-Smith and Richard Le Mesurier who have huge global experience and were convinced that there was a crying need for this device, especially in Africa. I was also fortunate to be linked early on with the IAPB who also saw its potential.
The device is already having a positive impact – and that’s great – but we’ve only scratched the surface. Health workers need a package with education posters and vital hands on instruction, model eyes to practice on, as well as ongoing mentorship. Implementation in developing countries is the “nut to crack” – easy to say and hard to do. Here in the UK, I use the device every day. It is particularly useful with children, as it is less “scary” and medical looking than the traditional ophthalmoscope. The basic format of the device has leant itself nicely to new add-ons: a smartphone clip (that costs pennies) for images and videos, a polarized dermascope attachment, and a “lenser” beam concentrator for hands-free ENT inspection with a simple headband. Our view is that simple, low-cost, easy-to-use scopes let users make quick on-the-spot common pathology diagnoses – ideal for patients and the wider community in remote areas, and also the health worker’s own confidence and knowledge. Telemedicine imaging has its place, and can be part of the mix for teaching and opinions on rarer cases. You won’t be surprised to learn that I’m now applying the same design concepts to more eye and ear devices...
William J Williams designed the Arclight, and is Director of Arclight Medical. He is an Honorary Research Fellow at St Andrews University, and an optometrist based in Liverpool, UK. John Sandford-Smith reports no conflicts of interest relevant to the content of this article. Andrew Blaikie reports that he is seconded to the University of St Andrews from NHS Fife. The University owns a social enterprise subsidiary company, for which Blaikie acts as an unpaid adviser, which sells the Arclight to users in the UK & Europe with profits being used to fund distribution and education exercises of the device in low income countries via the Global Health Implementation team at the University of St Andrews. William J Williams is Director of Arclight Medical. Credit for Arclight images: Andrew Blaikie, William J Williams and Clare Morton.
Making a Difference Globally by John Sandford-Smith Getting the Idea Out There by Andrew Blaikie Bringing the Idea to Life by William J Williams
