So this is about cataract complications, and you know, those videos that the Canadian Choppers showed, c’mon, anyone could do that. That’s easy stuff – baby talk! I wanted to present something that we see all the time. This might not be sexy, but it’s very relevant.
A. The case I’m presenting is one of a 59-year-old hyperope who had phacoemulsification with a toric lens. Postop day one she’s great, a week later she comes back and her vision has decreased – the toric has rotated 43 degrees!
B. I brought her back to the OR two weeks later and repositioned the toric lens with intraoperative aberrometry once again. The day after surgery, her vision was wonderful! A week later, she comes back and it has rotated again – 37 degrees.

C. Now remember she’s a hyperope. We’ve seen these cases before but usually the patients are axial myopes – they keep rotating, you keep repositioning, and your patient keeps coming back again and again... so what should I do?
D. If you believe in some higher power, are you going to re-rotate and pray? Or what about a reverse optic capture?
E. How about placing a CTR? Lots of authors have published on this, but the problem is that even after the insertion, the IOL can still rotate. How about inserting two CTRs? Sagiv and Sachs reported that implanting two can stabilize the toric IOL.
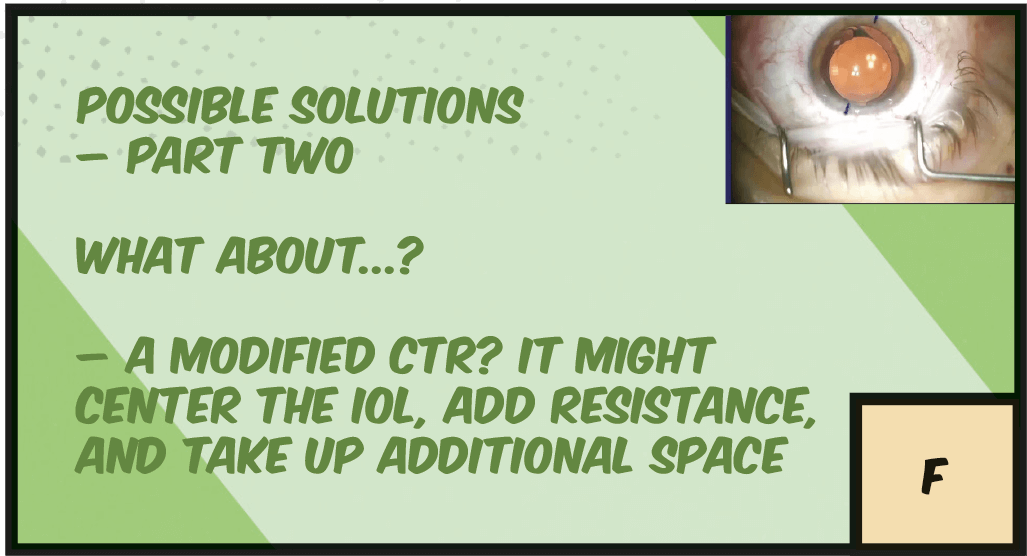
F. Another option is to place a modified CTR. The idea being that the CTR centers the lens, and takes up additional space, while the indentations in the modification will hopefully hinder the rotation even more by adding resistance.
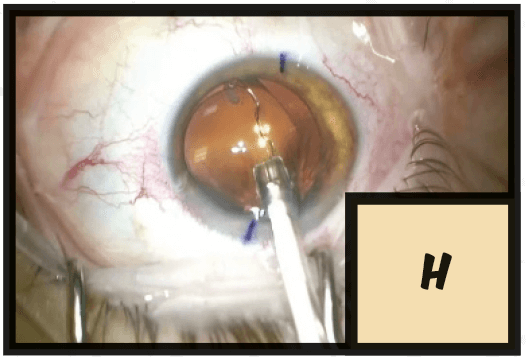
G. One tip is to inject the modified CTR counter-clockwise, because if injecting clockwise, you can inadvertently capture the CTR in the haptic-optic junction.
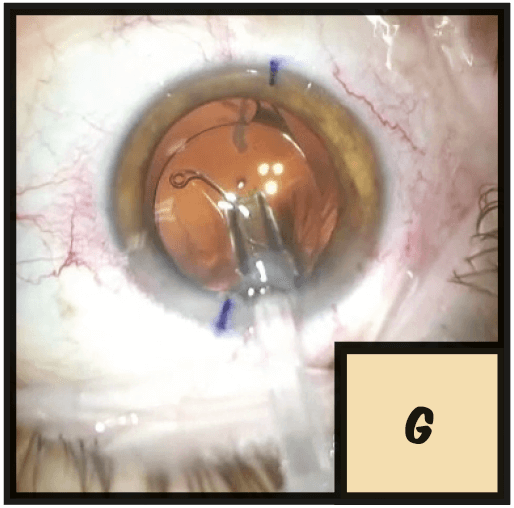
H. If you insert it counter-clockwise, the CTR will be inserted in the same direction as the haptic, and therefore it is harder to become trapped in the haptic-optic junction which can move the IOL out of position.
I. After the second rotation and placement of modified CTR, the toric IOL stayed in position and the patient did well.
J. In conclusion, when a toric IOL rotates, placing a CTR can help stabilize the position. And remember, toric IOLs can rotate off-axis even in hyperopes. It is common to associate myopes with long anterior chamber depths and rotating IOLs. And in fact, this patient did have a pretty long anterior chamber depth, but a short axial length, which threw us off. So fixing a roulette wheel toric with a modified CTR can really lead to hitting the jackpot!
Captain Ectopia (Lentis) Ninja-ing In and Out of a Tight Spot
